Inflammation, edema, and pain in the young adult patient are always indications for the extraction of the mandibular third molar tooth bud during its emergence. The clinician will observe both by physical examination and a panoramic radiograph that the lack of space will inhibit the complete emergence of the tooth with normal dental and periodontal characteristics. At this stage of eruption, extraction is sometimes associated with complications resulting from infection. In addition, the surgical procedure may prove to be intricate, or even difficult, because of the nature of the complete root formation and root morphology in relation to the mandibular canal. Moreover, the periodontal environment of the second molar may be compromised by the resorption of the alveolar wall of its distal root. It is therefore preferable to extract before these problems arise.
At what age should treatment start?
According to clinicians, the best time to carry out germectomy is during one of the three stages of tooth development. The orthodontist will develop a treatment strategy that will determine when the surgical phase should be undertaken. Dental age and bone age do not always correspond to chronological age because in some children calcification of the tooth bud occurs early, while in others it may be delayed for several years (Parant).
First stage: 7 to 11 years of age, beginning of tooth bud calcification
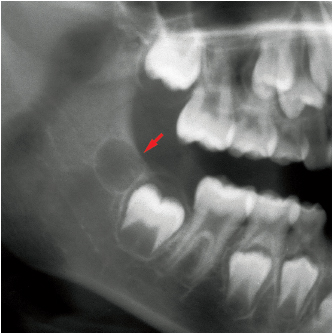
The bone crypt of the third molar is well defined by the age of 5 to 7 years and is usually located near the anterior border of the ramus. Germectomy carried out at this stage is therefore considered by some authors to be a simple curettage (Asanami and Kasazaki). The bone crypt is open and its contents are enucleated as soon as calcification of the dental organ begins (Figs 7-1 and 7-2).
It should be re-emphasized that it is difficult to assess the amount of space that will be available for the development of third molar before the end of growth because this space increases with the remodeling resorption of the anterior border of the ramus (Ten Cate).
Early germectomy (before the end of crown calcification) is therefore not desirable. Indeed, it is a surgical procedure which, if carried out at the onset of adolescence, may have significant psychological effects regardless of whether local or general anesthesia is used. This procedure cannot be totally risk free and thus it is difficult to justify its use.
Second stage: 12 to 15 years of age, crown mineralization is complete
The earliest crown calcifications do not begin before the age of 10 years. Around the age of 14 years, root formation has only just begun. At this stage of tooth development, the roof of the bone crypt is not fenestrated. Opening the crypt surgically is rarely satisfactory, and the tooth bud tends to pivot easily on itself. The crown, which by this stage has reached its final dimensions, should always be sectioned.
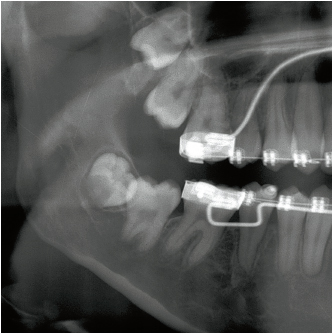
Germectomy may be included in an orthodontic treatment strategy when extra space is required in the posterior areas (Fig 7-3). Germectomy may also be carried out to ensure that the second molar erupts in a completely upright position, or when the orientation of the tooth bud is significantly abnormal (Figs 7-4, 7-5a, and 7-5b).
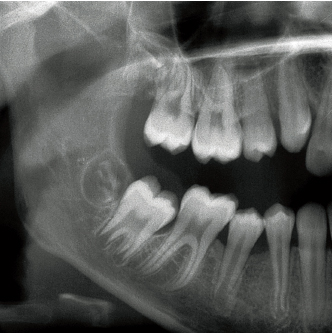
7-2 Crown mineralization has just started in this 12-year-old male patient. The age at which each developmental stage of the third molar occurs varies among patients.
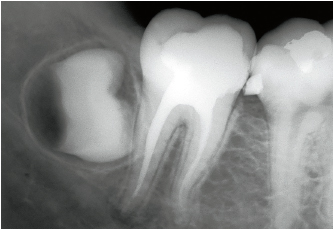
7-3 This radiograph of the occlusal face of the right mandibular third molar shows that the tooth bud is growing in a transverse direction. The precise orientation of the tip of the crown cannot be determined from this radiograph.
7-4 It is clear that this tooth bud (right mandibular third molar) will not be able to achieve an upright position. It therefore may be best to consider germectomy before the roots begin to develop.
Third stage: 14 to 18 years old, root formation is partially complete
The so-called eruption only begins when the second third of the root becomes calcified(Kor/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


