6
Radiographic Analysis of Anomalous Tooth Forms and Morphological Variations Related to Endodontics
An anomaly is a marked deviation from normalcy, especially as a result of congenital or hereditary defects. Recognition and endodontic treatment of dental abnormalities can present a challenge to every practitioner. Radiographic evaluation during a consultation visit is a key element in the pretreatment assessment of a patient’s “degree of difficulty” (CAE, 1998). Determination of the complexity of treatment and assessment of the physical nature and condition of a tooth to be treated allows the practitioner to better prepare before treatment commences.
Dens Evaginatus
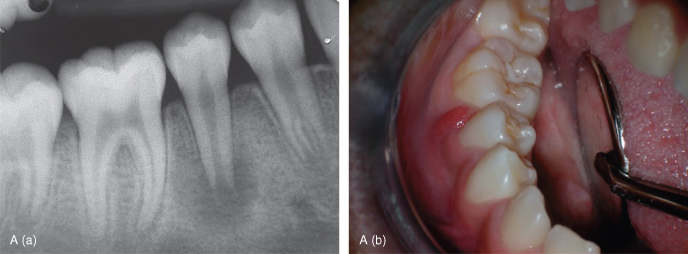
The dens evaginatus is a developmental anomaly that manifests clinically as an extra cusp appearing on the occlusal surface of premolar teeth between the buccal and lingual cusps (Figure 6.1). This projection of enamel can interfere with tooth eruption and occlusion. This tubercle is usually worn down or broken off, which can result in pulp exposure, and subsequent pulp necrosis and periradicular periodontitis (Figure 6.2A). Radiographically, this condition may be recognized by examining the radiodensity stemming from the cusp of the premolar crown tip before eruption (Figure 6.2B–D), which can influence orthodontic treatment planning (McCulloch et al., 1997). As a tooth is erupting, this extra cusp can also be seen radiographically as well as clinically (Figure 6.2E)
Figure 6.1 Projection of the extra cusp on the occlusal surface of the lower bicuspid tooth is seen clinically.
(Image courtesy of Dr. Raymond Greenfeld.)

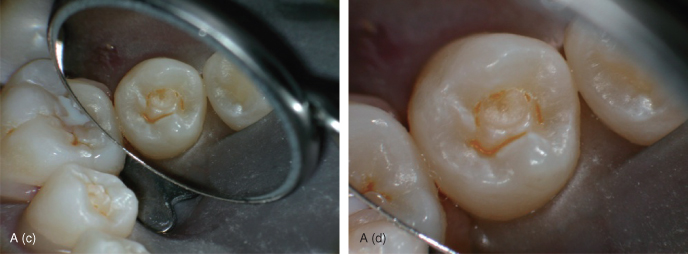
Figure 6.2 A. (a) Periapical lesion associated with the mandibular right premolar tooth. A slight thickening of enamel is seen in the center of the crown near the occlusal surface in the vicinity of the evagination. (b) Clinical view of lower right posterior teeth. The dens evaginatus tubercle has been either broken off or worn down on this second premolar tooth. (c) Occlusal view of the worn tubercle. (d) Magnified view of (c). B. (a) Panorex film showing multiple dens evaginatii of unerupted mandibular premolar teeth. Note the thin radiodensity of enamel near the center of the crown near the occlusal surface. All four unerupted mandibular premolar teeth show this radiolucency stemming from their cusps. Such radiodensities exhibiting this condition are not easily seen on the maxillary premolar teeth. (b) Clinical photo after mandibular premolar teeth have erupted, showing dens evaginatus occurring in all four lower premolar teeth
(Images courtesy of Dr. Angelina Loo).
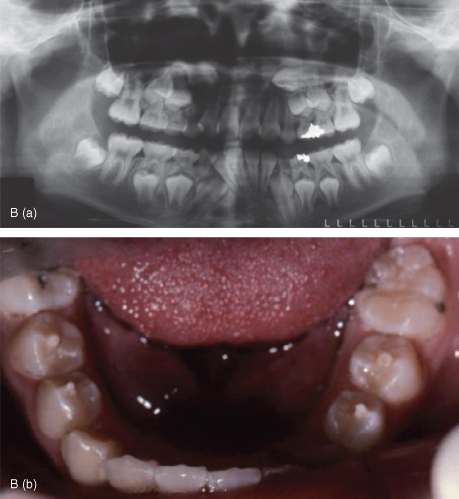
C. Panorex films showing (a) pre- and (b) posteruption states of this patient’s dentition. (c) Breakage of the tubercle on the lower right second premolar tooth necessitated a pulp cap and restoration of this tooth
(Images courtesy of Dr. Angelina Loo).
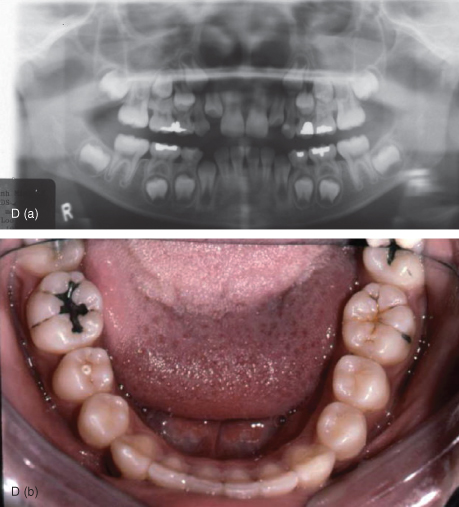
D. (a) Panorex film exhibiting dens evaginatus on both unerupted lower second premolar teeth. (b) Clinical view of erupted teeth exhibits the protruding dens evaginatus along the lingual ridge of the buccal cusp of the lower right second premolar tooth. Note the “target-like” appearance of this worn tubercle indicative of enamel (outer) and dentin (inner) components. The occlusal surface of the left second premolar has a worn tubercle also, but it does not have this same appearance indicating only an enamel involvement
(Images courtesy of Dr. Angelina Loo).
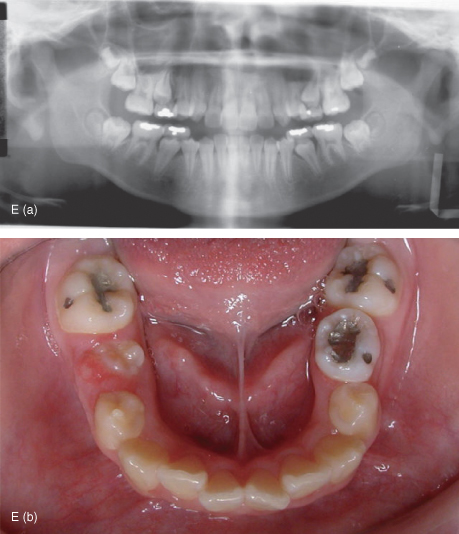
E. (a) Panorex film showing an erupting lower right first premolar tooth. A typical dens evaginatus seen as a radiodensity stemming from the clinical crown is evident. (b) Clinical view of this partially erupted tooth shows an obvious tubercle associated with the clinical crown
(Images courtesy of Dr. Angelina Loo).
Dens Invaginatus
This malformation of teeth usually affects maxillary lateral incisors, and is considered to be an invagination of the dental papilla during development. Although the etiology remains unclear, this tooth abnormality has been described for hundreds of years (Hulsmann, 1997). Various types of this invaginated tooth anomaly were characterized by Oehlers (1957). He categorized this malformation to occur in three different forms as shown in Figure 6.3.
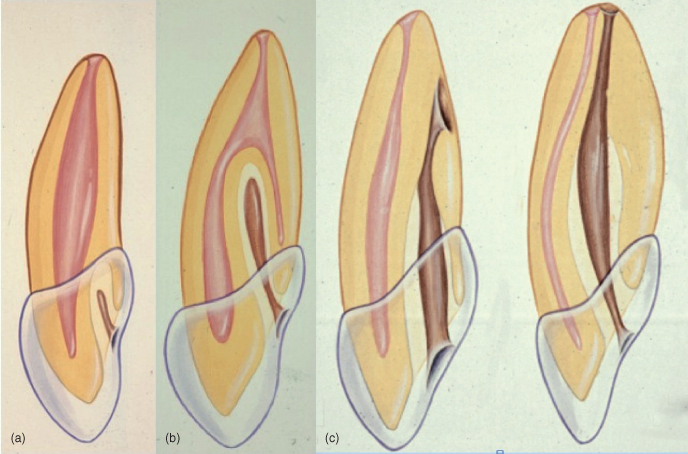
Figure 6.3 Categories of dens invaginatus as characterized by Oehlers (Oehlers, 1957). (a) Class I is an invagination that is limited to the crown of the tooth. (b) Class II invaginations extend beyond the CEJ into the root, but end as a blind sac. (c) Class III invaginations extend deeper into the root and communicate with the external root surface and may extend to the apical root third. Note that none of these invaginations directly communicate with the pulp.
(Images courtesy of Dr. Raymond Greenfeld.)
The first type of dens invaginatus, Class I, is a minor form of an invagination that occurs within the crown of the tooth, and does not extend beyond the cementalenamel junction (CEJ). It can be seen radiographically as an invagination in the vicinity of the cingulum (Figure 6.4).
Figure 6.4 Dens invaginatus Class I. Radiodense projections are seen emanating from the cingulum of these maxillary central incisor teeth.
(Images courtesy of Dr. Raymond Greenfeld.)

Deeper forms of invagination that cross the CEJ and invade the root, yet still end in a blind sac, are categorized as Class II. Such invaginations are shown in Figure 6.5. These invaginations may or may not communicate with the pulp. Radiographically, these may appear as a “dens in dente” (tooth within a tooth), although this is a misnomer. It is recognized as a pear-shaped invagination emanating from the crown of the tooth (Figure 6.6). There is a constriction at the beginning of the invagination on the surface of the tooth, before it expands deeper into the root. It may appear that the invagination goes into the pulp because of the superimposition of the invagination over the root canal (Figure 6.7a). Food, bacteria, and debris may get packed into the opening of the invagination, resulting in caries and communication with the pulp. Sealing off the invagination with a bonded resin is shown in Figure 6.7b,c.
Figure 6.5 Dens invaginatus Class II. (a) Double invagination of the upper left maxillary incisor tooth extending below the CEJ. (b) Invagination near the incisal edge of the upper right maxillary lateral incisor extends below the CEJ and appears directly adjacent to the root canal space.
(Images courtesy of Dr. Raymond Greenfeld.)
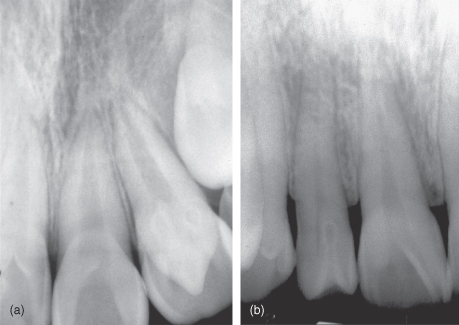
Figure 6.6 Ground section of a tooth exhibiting dens invaginatus Class II. This image shows how this malformation appears like a tooth within a tooth, “dens in dente”
(Image courtesy of Dr. Ravindra Shah).
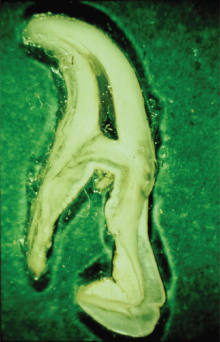
Figure 6.7 (a) Dens invaginatus Class II. Radiographically, the invagination is superimposed over the root canal in this upper right lateral incisor tooth. The pulp in this tooth responds normally to thermal testing. (b) Pre- and (c) posttreatment using an acid etched and bonded resin to seal off the invagination.

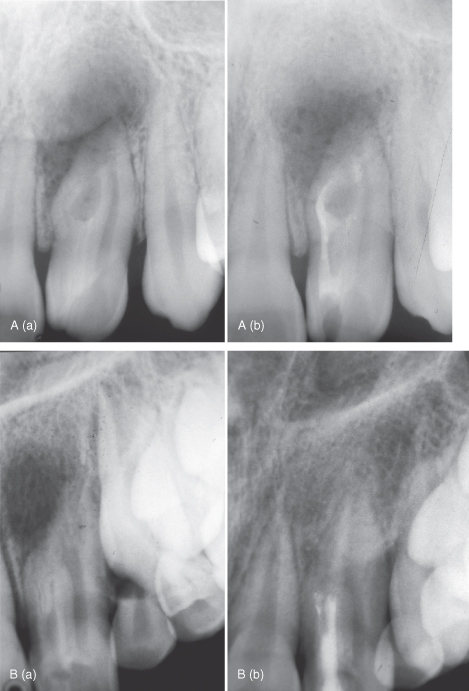
Still more severe forms on the invagination, penetrating to communicate with the external root surface and extending to the apical root third, can have quite a malformed appearance (Figure 6.8A). Although this Class III invagination is extensive, there is usually no immediate communication with the pulp. Figure 6.8Ba shows a maxillary lateral incisor tooth with apical periodontitis resulting from infection originating from an invagination. The pulp responded normally to thermal testing. A recall radiograph shows healing of the apical periodontitis, and clinical examination revealed that the pulp continued to respond normally to pulp testing procedures.
Figure 6.8 A. Dens invaginatus Class III. (a) Pre- and (b) posttreatment radiographs showing an upper left lateral incisor tooth with associated periradicular radiolucency. This tooth responded normally to pulp testing procedures before and after treatment of this invagination
(images courtesy of Dr. Raymond Greenfeld).
B. A complex anomaly involving dens invaginatus Class III and either fusion or gemination. Notice that the preoperative radiolucency of the upper left lateral incisor (a), resolved after treatment of the invagination (b). This tooth responded normally to pulp testing procedures before and after treatment of this invagination.
(Images courtesy of Dr. Raymond Greenfeld.)
Fusion
Fusion is the result of the union of two separate tooth germs. If contact occurs early in development, before calcification begins, two teeth may be united to form one large tooth (Figures 6.9 and 6.10). Radiographically, this can be seen as one large root and root canal system, while having a malformed crown (Figure 6.11). Such clinical presentations have significant orthodontic implications.
Figure 6.9 (a) Clinical view of fused mandibular anterior teeth. (b) Fusion involves both the crown and root, as seen here.
(Images courtesy of Dr. Ravindra Shah.)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


