Chapter 6
I’ve Got a Locking Joint
History
Katie is a 16-year-old schoolgirl who comes into your surgery in a panic with her mum first thing in the morning. She says that her jaw is locked on the right side and she can’t open her mouth beyond a couple of fingers’ width. She has tried to force her jaw open but this was extremely painful and she couldn’t manage it.
Previously she had had intermittent clicking for about 6 months.

She had mentioned this to you at her routine examination but at that time the click was not present and you suggested that she should report back to you if it became a problem. She wasn’t aware of what had caused the click but said that it had had a gradual onset with no particular initiating event. Over the last week she had been aware of intermittent locking on waking in the morning but this was always momentary and freed spontaneously within a few seconds. This morning she woke with her jaw locked. It did not free up as usual and has been locked since. She commented that since her jaw was locked the click had now gone but her jaw was very painful. She is really worried as she has exams soon and she said ‘I don’t need this just now’.
She is worried not only about the pain but also about how any treatment will interfere with her studies. She attended with her mother who expressed concern about how you were going to help her today, in the immediate future and what the potential for this happening again was. Apart from her TMJ click there was no relevant previous medical or dental history.
Examination
Katie has a class I, basal bone and incisal relationship. She appeared anxious but said that when she was at rest she was not in much pain. The discomfort was present only when she tried to open her mouth beyond a certain point (Figure 6.1).
Figure 6.1 Locked right TMJ with lasting mandibular deviation.

You examined the TMJs for tenderness. There was no tenderness on lateral palpation but there was tenderness on intra-auricular palpation on the right-hand side. You palpated and listened to the jaw joints for sounds; there was no evidence of clicking. You palpated the masseter, lateral pterygoid and temporalis muscles, but there was no tenderness. Katie did comment that when she bit hard together she experienced pain in her right ear. You asked her to open her mouth and you examined her pathway of jaw movement. She could open comfortably to 17 mm, at which stage she said her jaw ‘would not go any further’. At this point, when she did try to force her mouth open further, her mandible deviated across toward the right-hand side. She said that she felt that this was because there was something ‘getting in the way’. Her limitation of mouth opening was therefore not purely due to pain – there was also a physical obstruction.

Radiographs/Imaging 
Katie asked you to take a radiograph because she wanted to see what was wrong. You declined to do this because you knew that a radiograph would not give you any more information and would not even confirm your clinical diagnosis.
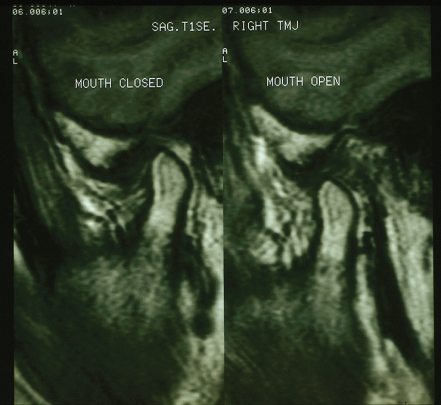
Further imaging such as MRI (Figure 6.2) might be suggested but only if an invasive, possibly surgical treatment plan was being contemplated, otherwise there is no indication for such a test.
Figure 6.2 A magnetic resonance scan showing the condyle–disc relationship.
Diagnosis
The diagnosis in Katie’s case is one of an internal derangement in the TMJ of disc displacement without reduction. When considering this definition think of the word ‘reduction’ in an anatomical way – a structure going back into place – and do not link the word reduction with reduced movement. A useful analogy is, if a shoulder joint has been dislocated, reduction of this dislocation means that the joint components are repositioned to their anatomically correct position. The correct definition of clicking is disc displacement with reduction, i.e. the disc reduces to a normal position whereas in locking this does not happen, hence the term ‘disc displacement without reduction’.
The main complaint is one of an inability to open the mouth beyond a certain degree due to a physical obstruction. Patients with this condition frequently report that trying to open their mouth causes a feeling like stretching an elastic band in the joint.
They can close their mouth freely but biting together can be painful. The reason for this is that, when a patient with an anteriorly displaced disc bites firmly in centric occlusion, as the disc is displaced forward, the highly innervated elastic posterior portion of the disc becomes inter/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


