CHAPTER 5 Prosthetic Options That Influence Implant Selection
The patient will have either a completely or partly edentulous arch. Either condition may be restored with removable, fixed-detachable (removable only by the dentist), or cemented prostheses, which are placed directly into or onto the implant or implants or onto a bar that has been attached to them. Implant-borne prostheses often consist of two separate parts: mesostructure bars and superstructures (Figs. 5-1 and 5-2). Superstructures are the final or tooth-bearing part of implant prostheses. They may be single crowns, complete overdentures, or any of the variety of prostheses in between, such as fixed bridges, fixed-detachable bridges, or combinations. Overdentures sometimes are attached to coping bar splints; these splints are called mesostructures. Mesostructures can be affixed to implants or implant-tooth combinations.


When planning the final restorations, the implantologist should determine whether the prosthesis is intended to replace teeth, teeth and soft tissue, or teeth, soft tissue, and bone. The more soft tissue and bone to be replaced, the greater the height of the restoration must be. Depending on the amount of hard and soft tissue that must be replaced, more implant support is required in direct relation to the size and height of the prosthesis. Restorations supported solely by implants always require a greater number of implants than do prostheses supported by both implants and soft tissue. Implant therapy allows for use of the prosthodontic options described later in Chapter 19.
SUPERSTRUCTURES
Overdentures
Overdentures can be classified into two types: those supported by soft tissue and implants or teeth and those supported purely by implants. Overdentures supported by soft tissue and implants or teeth are supported by the implants and soft tissues and retained by the implants. For this to be practical in the parasymphyseal area, the retainers (implants or teeth) must be in a position that allows construction of a straight bar (Fig. 5-3). With this arrangement, several internal clips can rotate around the bar, which allows the posterior overdenture saddles to be soft tissue borne, so that they may take some of the stress from the implants or teeth. If the bar is placed in the anterior region and, because of the location of the implant or implants, must be curved to conform to the shape of the arch, the overdenture does not rotate on the bar, and the posterior saddles may act as levers, tending to loosen the retaining screws, cement, abutments, or the implants themselves (Fig. 5-4).
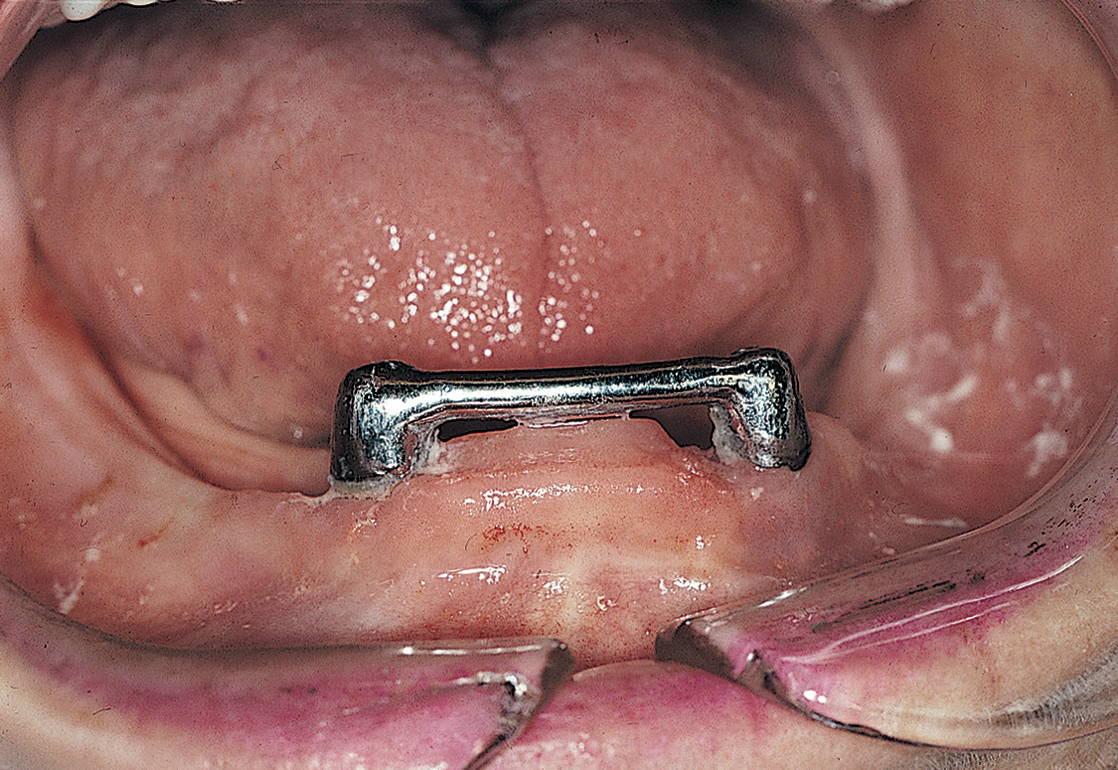
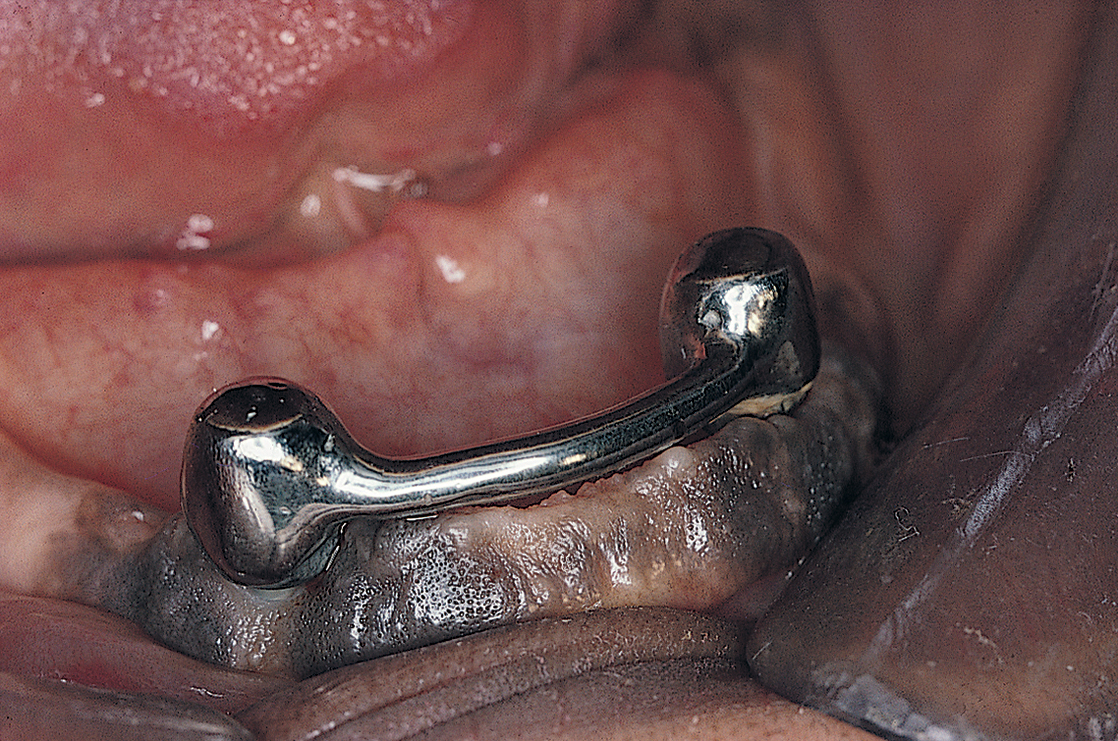
FIGURE 5-4. When splinting implants require a curved bar, the superstructure attachment must permit rotation (i.e., “sloppy fit”) to allow for tongue space (see Fig. 5-15).
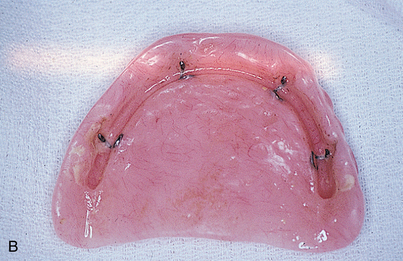
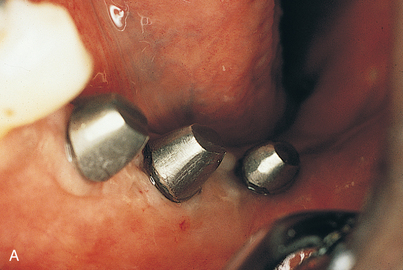
From an engineering standpoint, splinting implants with bars and copings, rather then using them individually, is preferable. Mesostructure bars are available in various shapes and configurations, and the type used depends on the location, length, and number of implants to be placed; the percentage of surface area surrounded by bone (osseointegration); and the type of retention devices selected (e.g., Locators, clips, O-rings, Zest, Ceka, ERA). Bar-borne overdentures are both supported and retained by their bars (Figs. 5-5 and 5-6), which in turn should be supported by four or more root form implants 10 mm long or longer, by transosteals, or by subperiosteal implants.


Fixed Bridges
Fixed bridges may be supported completely by implants, or they may be used in conjunction with natural tooth abutments (Figs. 5-7 and 5-8). In both cases, construction begins after transepithelial abutment (TEA) placement (by spline, frictional fit, or threading) and is completed with the implantologist’s preferred prosthetic techniques. Various attachments or interlocks between the implants and the natural abutments may be chosen (e.g., DE Hinges, Dalbo, Crismani, Mini Rest, Tube and Screw). These provide stress-breaking features that may be important, because the support mechanisms differ so dramatically between implants and natural teeth.

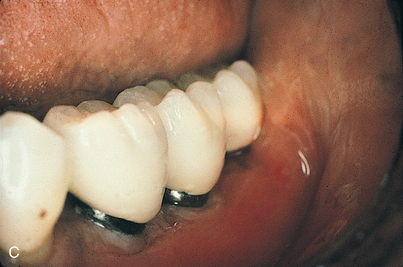
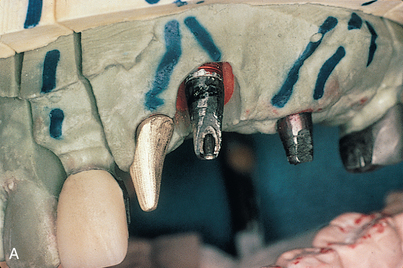
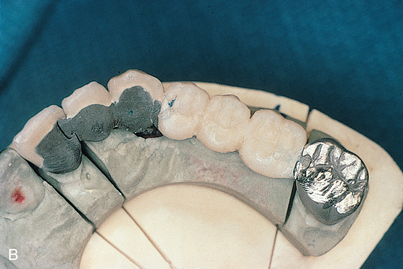

Fixed-Detachable Bridges
The fixed-detachable bridge is a prosthesis that can be removed by the dentist but not by the patient. Screws attach the bridge to the implants, to their abutments, or to an interposed mesostructure bar. These prostheses most often are completely implant borne (Fig. 5-9). However, natural tooth abutments may be incorporated into implant bridges through the use of semiprecision attachments or internally threaded telescopic copings (Fig. 5-10). The techniques used to produce fixed-detachable bridges are by far the most complicated, and the opportunities for error are numerous. (Before selecting this method, the implantologist should review chapters 22, 23, and 24.) The benefits of being able to remove these bridges must be balanced against the difficulties involved in their fabrication, the cost, the potential for postinsertion complications, and the restoring dentist’s willingness to manage them.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


