5
Orthognathic technical procedures
- Have a working understanding of face bow recordings and their anatomical importance, the use of articulated dental casts for surgical prediction including measurement of movements, construction of occlusal re-positioning wafers and the use of 3D models in surgery planning.
5.1 Introduction
The role of the maxillofacial technologist as a member of the team treating patients presenting at a dento-facial deformity clinic can be easily defined. The technologist will use clinical measurements of the hard and soft tissues to reproduce the planned prescribed surgery on anatomically positioned dental casts in three dimensions. This procedure will allow the surgical team the opportunity to examine the predicted surgical outcome and allow re evaluation of the plan should this be required. Perhaps the most important aspect of the model surgery is the construction of intra operative occlusal wafers in final and intermediate positions used to reposition the upper and lower jaws at the time of surgery.
The opportunity to see the patient by the technologist responsible for the model surgery is essential and invaluable. The technologist can visualise the degree of correction required to treat the patient, this can include the amount of maxillary tooth show, whether there is an occlusal cant present or indeed any facial asymmetry which needs to be considered when formulating the treatment plan.
Once the plan has been formulated and agreed with the patient it will be necessary to formalise the model surgery with some anatomically accurate models and clinical measurements of the patient.
5.2 Clinical assessment
At the surgery planning appointment the following must be obtained in order for an anatomical model surgery plan to be carried out.
Figure 5.1 Patient planning sheet.
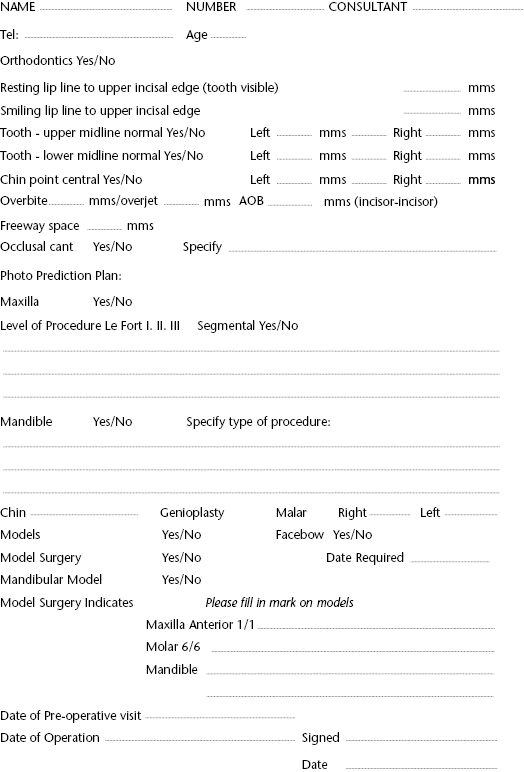
5.2.1 Patient planning sheet
The first stage in this process is to record the patient’s soft tissue and dental measurements on a treatment planning sheet. This will ensure the patient’s individual details are accurately recorded to allow model surgery to be carried out. Details in addition to those previously mentioned include the dental centre lines, chin point, freeway space, overjet and overbite and are amongst the relevant items of information to be recorded; a clinic during which several new patients have been seen may be vivid in one’s memory on the day, however, this will be less so a few days later and the planning sheet should avoid confusion in this regard. Additional information should include patient contact details in case it is necessary to recall them for further clinical assessment.
5.2.2 Master impressions
The technologist must be given the opportunity to examine the final impressions for quality control and must ensure the impressions are not loose in the tray. All present teeth must be included, often wisdom teeth can be missed or be only partially present in the impression. These teeth may be in occlusion and their omission may well cause problems when re-positioning the jaws during surgery therefore care at the impression stage is essential. The selection of impression material is a question of operator choice but it must provide accurate models. If circumstances are such that the impressions cannot be cast quickly a dimensionally stable material such as a rubber based product must be used. The choice of impression tray is also critical and this must be capable of withstanding the difficulties associated with the removal of the impression when orthodontic attachments are present on the teeth. The orthodontic attachments often tear the impression material or separate it from the impression tray rendering it useless, under these circumstances the impression must be repeated until a suitable one is taken. The best types of impression tray are the fine perforated metal trays or the disposable orthodontic trays specifically designed for orthodontic impressions. The impression can be checked by turning it over to the tray side to ensure it is firmly attached, if not it must be rejected. The technologist will invest two or three working days on the pre-op master models obtained from the impressions so must be satisfied they are fit for purpose.
Figure 5.2 Impressions resting on a support.

5.2.3 Occlusal registration
A registration of the patient’s occlusion should be taken at the clinical appointment and similarly should be carefully checked for accuracy. Once again the selection of registration material is operator choice. In addition to wax there is a large selection of silicone based materials formulated for bite registration purposes available. It is worth noting the reason for most discrepancies occurring between the prediction planning and the model surgery, these tend to be as a result of inaccurate occlusal registrations so it is always worth taking the time to double check the accuracy of the bite record.
5.2.4 Face bow recording
Finally a face bow registration should be taken if required. This must be taken by an experienced member of the team used to the procedures of face bow recordings. The face bow is the foundation of model surgery and inaccuracy at this stage may be transferred to the patient’s intra-operative positioning wafer and subsequently it will have a detrimental effect on the patient’s post-operative outcome. The face bow recording procedure is described later in this chapter.
5.3 Articulator and face bow selection
Orthognathic model surgery plays an important part in the diagnosis and treatment of the dento-facial deformity patient. There are many differing techniques and methods of model surgery used by the maxillofacial technologist within the laboratory environment, many of which are employed as a result of a particular departmental or operator preference or are simply historically employed techniques handed down from technologist to technologist. In today’s practice evidence based techniques are required to comply with health care policies. The inherent problems with face bow registrations and articulator selection have been well documented in the literature. Before considering the selection of the appropriate articulator for a given procedure it should be noted from the outset that the instruments in use today are dental in origin and were not designed for orthognathic model surgery, thus criticism of their inadequacy is inappropriate and the technologist must be prepared to modify techniques to compensate for their inaccuracy.
5.3.1 Plain line articulator (simple hinge)
The simple hinge articulator or plain line articulator as it is more commonly known is the most basic dental articulator capable of only opening and closing from a fixed hinged axis point. Dental casts are mounted between the top and bottom arm in an arbitrary position. There is no anatomical orientation to the skull with the exception of the occlusal relationship of the upper and lower teeth.
This can be used successfully for some single jaw osteotomies and segmental procedures typical applications would include:
5.3.2 Semi-adjustable articulators and face bow recordings
For patients requiring surgery on both the upper and lower jaws (bi-maxillary procedures) to correct a facial deformity or for maxillary surgery requiring height changes, the use of a semi-adjustable articulator is essential (Figure 5.3). This principle applies to all bi-maxillary procedures with no exceptions. The semi-adjustable articulator is used in conjunction with a face bow recording. This recording is used to orientate the dental casts of the patient on the dental articulator allowing pre surgical diagnostic assessments to be made.
Figure 5.3 Range of popular semi-adjustable articulators: left to right – Denar, KaVo, SAM, Hanau, Dentatus.

The principles of usage of a face bow recording and a semi adjustable articulator must be considered. The prosthetic application for which these instruments were designed must be re-evaluated as the anatomical points of interest for the correction of a dento-facial deformity differ significantly from those required for prosthetic dental restorations. The face bow recording must accurately position the maxillae in relation to the base of the skull. In addition the maxillary occlusal plane angle must be recorded precisely. Failure to record either of these with optimal precision will render model surgery inaccurate. It is important to remember that any inaccuracies incorporated into the model surgery will be transferred to the intra-operative repositioning splints and subsequently to the patient at the time of surgery producing a compromised surgical outcome.
5.4 Face bow recordings
Face bows commonly used for orthognathic model surgery will record the A.P. dimension of the patient with acceptable accuracy, however, most tend to overestimate the maxillary occlusal plane angle with dire consequences. These consequences will be discussed later in this chapter.
Firstly the available face bows should be considered to allow appropriate selection. The face bow is developed for individual articulators and as a rule should not be interchanged. Therefore it would not be wise to use for example a Dentatus face bow with a Hanau articulator regardless of the fact that Dentatus face bows fit the Hanau articulator and vice versa. Anatomical reference points differ depending on the manufacturer, but for the face bow to be of use for orthognathic model surgery it must record three points or planes of reference.
5.5 Face bow points and planes of reference
There are two commonly used types of face bow available for mounting casts on the semi-adjustable articulator. These are the auricular average value face bow and the condylar average value face bow.
5.5.1 Auricular average value face bow
The auricular face bow uses the external auditory meati as the posterior location. The maxillary dentition recorded on the bite fork which is attached to the face bow frame is the second recorded anatomical plane (Figure 5.4a). The third point of reference will vary depending on the manufacturer’s preference. This may be any of the points listed previously as face bow points of reference item 3. The auricular face bow finds favour as it is considered to give reproducible results due to the ease of locating the external auditory meati. It is, however, hard to see the relevance of the auditory meati in relation to mandibular deformity correction or maxillary cast positioning on the articulator. This type of face bow makes the assumption that the head of the condyle will be found in the arbitrary position of 13 millimetres anterior to the external auditory meatus. This assumption may be reasonable for patients with a symmetrical deformity. However, it is not appropriate for patients with craniofacial deformities such as hemifacial microsomia where the position of the condylar head will not be in a predictable position. A further disadvantage incorporated into some auricular face bows is the design of the bite registration fork. This fork is part of a removable jig which is detached from />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


