5 Orthodontics and Pediatric Dentistry
OUTLINE OF REVIEW
1.1 Epidemiology of Malocclusion
Prevalence
A. Crowding
B. Angle classification (see Orthodontic Diagnosis for definitions)
1. Overjet of > 5 mm, suggesting Class II malocclusion, occurs in 23% of children, 15% of adolescents, and 13% of adults.
2. Reverse overjet, suggesting Class III malocclusion, is much less frequent than Class II in the U.S. population (∼1%).
1.2 Growth and Development
Theories of Growth Control
Endochondral versus Intramembranous Bone Formation
A. Endochondral bone formation. Formed first in cartilage, then transformed into bone. Bones formed in this way are probably less susceptible to environmental influences during growth and are under more direct genetic control. The bones of the cranial base are endochondral.
B. Intramembranous bone formation. Formed by secretion of bone matrix directly within connective tissues, without intermediate formation of cartilage. Growth of intramembranous bones is more influenced by the environmental forces around them. The cranial vault, maxilla, and mandible are all examples of intramembranous bones.
Sites of Growth in the Craniofacial Complex
A. Cranial vault
2. At birth, the bones are widely separated by loose connective tissues at the fontanelles. Apposition of bone along the edges of the fontanelles eliminates these open spaces but the bones remain separated by the cranial sutures.
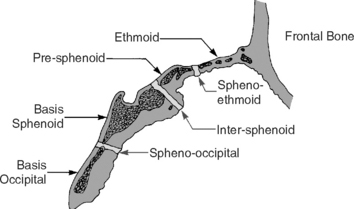
B. Cranial base
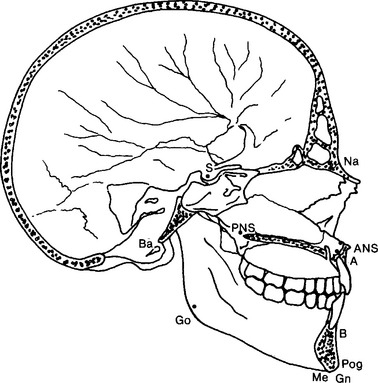
1. Ethmoid, sphenoid, and occipital bones (Fig. 5-1) at the base of the skull are formed initially in cartilage and later transformed into bone by endochondral ossification.
2. As ossification occurs, three bands of cartilage remain, which are important growth centers called synchondroses: the sphenio-ethmoid synchondrosis, intersphenoid synchondrosis, and spheno-occipital synchondrosis.
3. Each synchondrosis acts like a two-sided epiphyseal plate with growing cartilage in the middle and bands of maturing cartilage cells extending in both directions that will be replaced by bone.
C. Maxilla
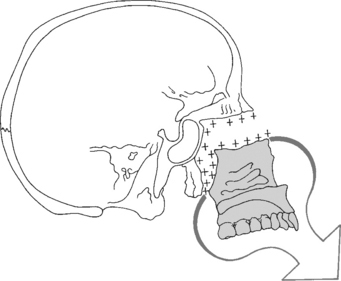
1. Growth of the maxilla is intramembranous. Growth occurs at the sutures posterior and superior to the maxilla at its connections to the cranium and cranial base, and by surface remodeling.
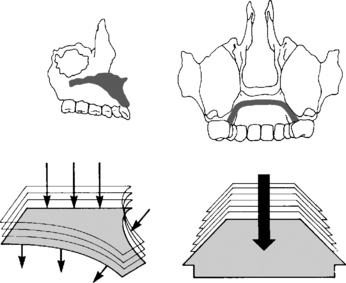
2. The maxilla migrates downward and forward away from the cranial base (Fig. 5-2), and undergoes significant surface remodeling (Fig. 5-3).
4. Much of the anterior movement of the maxilla is negated by anterior resorption, and downward migration is augmented by inferior apposition of bone.
5. As with all bones, interstitial growth within the mineralized mass of the maxilla is not possible; addition of new bone can only occur at the surfaces. Thus, increased space for the eruption of posterior teeth occurs by addition of bone posteriorly at the tuberosity as the maxilla migrates downward and forward.
D. Mandible
2. Cartilage covers the surface of the mandibular condyle at the TMJ. However, this cartilage does not grow independently like an epiphyseal plate or synchondrosis.
3. Cartilage is transformed into bone at the condyle as the mandible grows downward and forward, away from the cranial base. Surface apposition and resorption takes place in other areas of the mandible.
4. Most growth of the mandible occurs by new bone forming at the condyle and by resorption of the anterior part of the ramus with apposition posteriorly. Minor amounts of remodeling occur anteriorly and inferiorly.
5. Embryonic development
a. The mandible develops in the same area as the cartilage of the first pharyngeal arch—Meckel’s cartilage. However, development of the mandible itself proceeds just lateral to Meckel’s cartilage and is entirely intramembranous in nature.
6. As with the maxilla, interstitial growth within the mineralized mass of the mandible is not possible. Space for eruption of the posterior teeth occurs as the anterior portion of the ramus is resorbed extensively. Thus, in a child with crowded teeth it is not reasonable to expect that interstitial growth of the mandible will occur to create space within the body of the mandible to alleviate the crowding.
8. Mandibular growth rotation
a. As growth at the condyle facilitates movement of the mandible downward and forward, away from the cranial base, a gap is available between the maxilla and mandible in which the maxillary and mandibular teeth erupt.
b. Average closing rotation: in most children, condylar growth exceeds molar eruption and the mandible rotates slightly closed over time. This closing rotation, along with the downward and forward growth of the mandible itself, helps make the chin appear more prominent as children age. It also indicates that, in most cases, posterior face height increases more than anterior face height.
Timing of Growth
A. Cephalocaudal gradient of growth
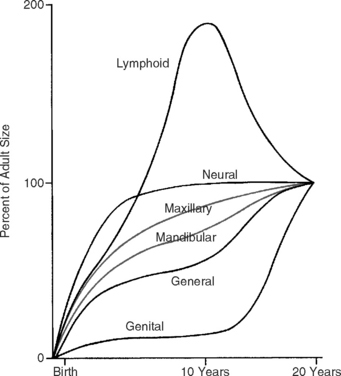
B. Scammon’s growth curves
1. Neural tissues, including the brain, continue to grow rapidly after birth and reach near 100% adult size by about age 6 or 7.
2. Lymphoid tissues, including tonsils and adenoids, also grow quickly, reaching twice the adult size by about age 10, and then involute during the pubertal growth spurt to reach adult size.
3. Genital or reproductive tissues do not grow much until puberty, and then rapidly increase to adult size corresponding to the time of the pubertal growth spurt.
4. General body tissues, including muscle and bone, grow rapidly after birth, then slow somewhat in growth during childhood, and then accelerate again at the same time as reproductive tissues proliferate.
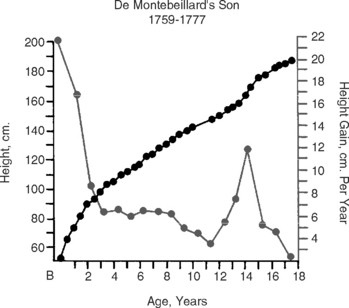
C. Growth velocity curve (Fig. 5-5)
1. The velocity curve shows that growth in height is very rapid after birth but decelerates quickly to a lower, more constant level in childhood.
D. Sex differences
1. Girls reach their growth peak about 2 years earlier than boys, on average. Average peak growth for girls is around age 12, for boys around age 14.
2. However, there is considerable individual variation in the timing of growth relative to chronological age, so that early-maturing boys may reach peak growth before late-maturing girls.
E. Predictors
1. Chronological age is not a perfect predictor of when peak growth will occur (correlation about 0.8).
2. Basing growth predictions on dental age is even less reliable (correlation about 0.7). In other words, children whose teeth erupt early do not necessarily grow early.
3. Physical growth status correlates well with skeletal age, which is determined by the relative level of maturation of the skeletal system.
a. A hand–wrist radiograph, revealing the ossification of the bones of the hand and wrist, is the standard for assessing skeletal development.
Cleft Lip and Palate and Other Developmental Abnormalities
B. Embryology
2. There are principal stages in craniofacial development. Some abnormalities in facial form and jaw relationships can be traced to malfunctions that occur during specific stages (Table 5-1).
| STAGE | TIME (HUMANS, POSTFERTILIZATION) | RELATED SYNDROMES |
|---|---|---|
| Germ layer formation and initial organization of structures | Day 17 | Fetal alcohol syndrome (FAS) |
| Neural tube formation | Days 18–23 | Anencephaly |
| Origin, migration, and interaction of cell populations | Days 19–28 | Hemifacial microsomia |
| Mandibulofacial dysostosis (Treacher–Collins syndrome) | ||
| Limb abnormalities | ||
| Formation of organ systems | ||
| Primary palate | Days 28–38 | Cleft lip and/or palate, other facial clefts |
| Secondary palate | Days 42–55 | Cleft palate |
| Final differentiation of tissues | Day 50–birth | Achondroplasia synostosis syndromes (Crouzon’s, Apert’s, etc.) |
(From Proffit WR, Fields HW, Sarver DM: Contemporary Orthodontics, ed 4, St Louis, Mosby, 2007.)
1.3 Development of Occlusion
A. Stages of normal dental development
2. The primary dentition stage
a. Starts with the eruption of the primary teeth and lasts until about 6 years of age, when the first permanent tooth erupts.
c. The mandibular anterior primary teeth are, on average, about 6 mm narrower mesio-distally than their successors.
d. Overbite, defined as the vertical overlap of the mandibular teeth by the maxillary teeth, develops as teeth erupt. Overbite can be measured in millimeters but it is preferable to measure it in percentages. Overbite normally varies from 10% to 40%.
e. Open bite is lack of overbite. Open bite or reduced amount of overbite is not unusual in children during the primary dentition due to habits such as thumb- or finger-sucking.
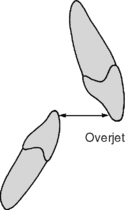
f. Overjet is the horizontal distance between the mandibular teeth and the maxillary teeth. Overjet normally varies from 0 to 4 mm. Habits will also cause an increase in overjet.
3. The mixed dentition stage
b. As each permanent tooth erupts, it is expected that its antimere (corresponding contralateral tooth) will erupt within 6 months.
c. “Ugly duckling stage.” As the two maxillary central incisors erupt, they move labially and a temporary diastema is often present between them. This has been referred to as the “ugly duckling stage” of the mixed dentition. When the permanent canines erupt, their mesial movement helps to close the diastema.
e. A transient open bite may be observed as a result of partial eruption of anterior teeth. Under normal conditions, the open bite will resolve with further tooth eruption.
g. Predicting molar relationship. According to Bishara (2001), during the transition period from the primary to the mixed dentition, cases with a flush terminal plane develop into a Class I in 56% of the cases and into a Class II in 44% of the cases. Cases with a mesial step relationship can transition into a Class I or, much less commonly, to a Class III molar occlusion according to their initial severity.
h. Normal characteristics of the mixed dentition. Molar and canine relationships are Class I; leeway space is present; well-aligned incisors or up to moderate crowding of the incisors; proximal contacts are tight.
i. Leeway space
(1) Defined as the difference in mesio-distal size between the primary canine, primary first molar, and primary second molar and their permanent replacements. The leeway space is larger in the mandibular arch, averaging 2.5 mm per side. In the maxillary arch, the leeway space is slightly smaller and measures about 1.5 mm per side.
B. Dimensional changes in the dental arches
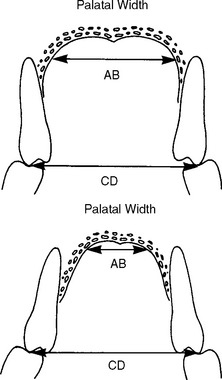
1. Width
a. The maxillary intercanine width increases by approximately 6 mm between the ages of 3 to 13. An additional increase of 1.7 mm occurs until the age of 45.
b. The maxillary intermolar width in the primary dentition increases 2 mm between the ages of 3 and 5 years. The permanent intermolar width increases by 2.2 mm between the ages of 8 and 13 years and decreases about 1 mm by the age of 45.
c. Part of the increase in width of the maxillary arch is due to the fact that the alveolar bone is divergent and, as growth and eruption occurs, the width increases.
2. Length
a. Arch length is a measure taken at the midline from a point midway between the central incisors to a tangent touching the distal surfaces of the second primary molars or the mesial surfaces of the first permanent molars.
3. Circumference (perimeter)
b. Measured from the distal aspect of the second primary molar (mesial aspect of the first permanent molar) on one side, and around the arch to the distal aspect of the second primary molar on the other side.
c. Mandibular arch circumference decreases significantly in the mixed to permanent dentition due to the mesial shift of the permanent molars into the leeway space, the mesial drift tendency of the posterior teeth in general, the slight amount of interproximal wear, and the lingual positioning of the incisors due to the differential growth of the maxilla (less) compared to the mandible (more).
C. Sequence of eruption
2. Primary dentition
3. Permanent dentition
b. The first permanent molar shows signs of calcification as early as the second postnatal month and the third permanent molar begins to calcify around the age of 8 to 9 years.
1.4 Orthodontic Diagnosis
A. Patient interview
Information to be sought during the patient/parent interview:
B. Oral examination
3. Dental/occlusal characteristics
b. Interarch (in three dimensions)
(1) Anterior-posterior (a-p)
(a) Angle classification
(i) Class I normal occlusion. Mesiobuccal cusp of the maxillary first molar in the buccal groove of the mandibular first molar and intra-arch relationships among teeth are correct.
(ii) Class I malocclusion. Mesiobuccal cusp of the maxillary first molar in the buccal groove of the mandibular first molar (but intra-arch relationships are abnormal).
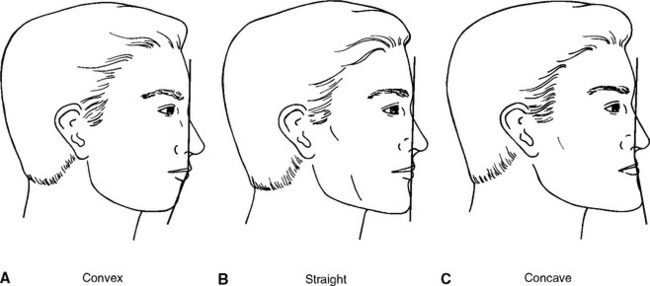
4. Facial esthetics/proportions
a. Frontal examination
(3) Lip posture (lip competence): with the teeth together and lips at rest, the lips should lightly touch or be slightly apart. A gap of more than 3 to 4 mm indicates lip incompetence because of a long lower face, protruding incisors, large overjet, or short lips.
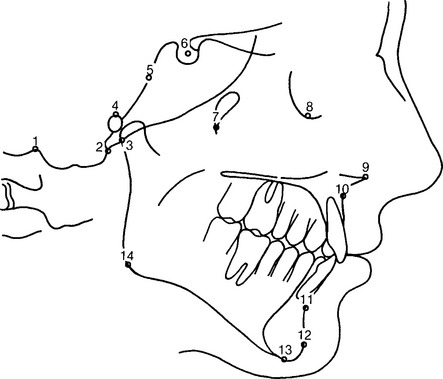
5. Skeletal relationships—cephalometrics
Cephalometric radiographs are standardized two-dimensional films of the skull. Subsequent films can be superimposed to evaluate growth and/or treatment effects. Individual films can evaluate dentofacial proportions or help clarify the anatomical basis for a malocclusion. This information should be used to confirm information from the clinical examination. Measures can be used to compare an individual to population norms, taking into account that there is much normal variation in the population.
c. Cephalometric measures
(3) ANB: A-P difference between maxilla and mandible: more positive indicates skeletal Class II; more negative indicates skeletal Class III.
(4) MP-SN: mandibular plane angle: bigger is steeper and indicates vertical growth pattern, with long lower face and anterior open bite tendency.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


