Criteria for Optimum Functional Occlusion
“THE CLINICIAN MANAGING THE MASTICATORY STRUCTURES NEEDS TO UNDERSTAND BASIC ORTHOPEDIC PRINCIPLES.”
—JPO
DORLAND’S MEDICAL DICTIONARY defines the verb occlude as “to close tight, as to bring the mandibular teeth into contact with the teeth in the maxilla.”1 In dentistry, occlusion refers to the relationship of the maxillary and mandibular teeth when they are in functional contact during activity of the mandible. The question that arises is: What is the best functional relationship or occlusion of the teeth? This question has stimulated much discussion and debate. Over the years several concepts of occlusion have been developed and have gained varying degrees of popularity. The development of these concepts is examined below.
History of the Study of Occlusion
In 1899 Edward Angle offered the first description of the occlusal relationships of the teeth.2 Occlusion became a topic of interest and much discussion in the early years of modern dentistry as the restorability and replacement of teeth became more feasible. The first significant concept developed to describe optimal functional occlusion was called balanced occlusion.3 This concept advocated bilateral and balancing tooth contacts during all lateral and protrusive movements. Balanced occlusion was developed primarily for complete dentures, the rationale being that this type of bilateral contact would aid in stabilizing the denture bases during mandibular movement. The concept was widely accepted; with advances in dental instrumentation and technology, it carried over into the field of fixed prosthodontics.4,5
As total restoration of the dentition became more feasible, controversy arose regarding the desirability of balanced occlusion in the natural dentition. After much discussion and debate, the concept of unilateral eccentric contact was developed for the natural dentition.6,7 This theory suggested that laterotrusive contacts (working contacts) as well as protrusive contacts should occur only on the anterior teeth. It was during this time that the term gnathology was first used. The study of gnathology has come to be known as the exact science of mandibular movement and resultant occlusal contacts. The gnathologic concept was popular not only for use in restoring teeth but also as a treatment goal in attempting to eliminate occlusal problems. It was accepted so completely that patients with any other occlusal configuration were considered to have a malocclusion and were often treated merely because their occlusion did not conform to the criteria thought to be ideal.
In the late 1970s the concept of dynamic individual occlusion emerged. This concept centers around the health and function of the masticatory system and not on any specific occlusal configuration.8 If the structures of the masticatory system are functioning efficiently and without pathology, the occlusal configuration is considered to be physiologic and acceptable regardless of specific tooth contacts. Therefore, no change in the occlusion is indicated. After examination of numerous patients with a variety of occlusal conditions and no apparent occlusion-related pathology, the merit of this concept became evident.
The problem facing dentistry today is apparent when a patient with the signs and symptoms of occlusion-related pathology comes to the dental office for treatment. The dentist must determine which occlusal configuration is most likely to eliminate this pathology. What occlusion is least likely to create any pathologic effects for most people over the longest time? What is the optimal functional occlusion? Although many concepts exist, the study of occlusion is so complex that these questions have not been satisfactorily answered.
In an attempt to determine which conditions seem least likely to cause any pathologic effects, this chapter examines certain anatomic and physiologic features of the masticatory system. An accumulation of these features will represent the optimal functional occlusion. This does not suggest that all patients must have these features to be healthy. As discussed in Chapter 7, there are great variations among healthy populations. However, these features should represent treatment goals for the clinician who plans to alter a patient’s occlusion for the purpose of either eliminating an occlusion-related disorder or restoring a mutilated dentition.
Criteria for the Optimal Functional Occlusion
As discussed, the masticatory system is an extremely complex and interrelated system of muscles, bones, ligaments, teeth, and nerves. To simplify a discussion of this system is difficult yet necessary if the basic concepts that influence the function and health of all the components are to be understood.
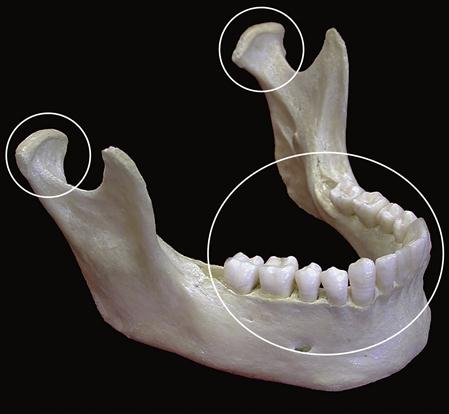
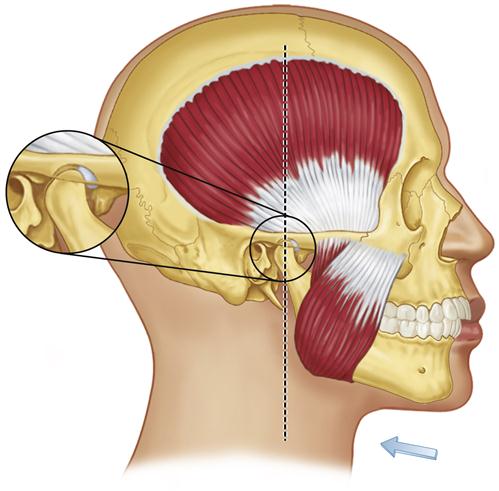
The mandible, a bone attached to the skull by ligaments, is suspended in a muscular sling. When the elevator muscles (the masseter, medial pterygoid, and temporalis) function, their contraction raises the mandible such that contact is made and force is applied to the skull in three areas: the two temporomandibular joints (TMJs) and the teeth (Figure 5-1). Since these muscles can provide heavy forces, the potential for damage to these three sites is high. Thus these areas must be examined closely to determine the optimal orthopedic relationship that will prevent, minimize, or eliminate any breakdown or trauma. In the following discussion, the joints and the teeth are examined separately.
Optimal Orthopedically Stable Joint Position
The term centric relation has been used in dentistry for many years. Although it has had a variety of definitions, it is generally considered to designate the position of the mandible when the condyles are in an orthopedically stable position. Earlier definitions described centric relation (CR) as the most retruded position of the condyles.9–11 Since this position is determined mainly by the ligaments of the TMJ, it was described as a ligamentous position. It became useful to the prosthodontist because it was a reproducible mandibular position that could facilitate the construction of complete dentures.11 At that time it was considered the most reliable, repeatable reference point obtainable in an edentulous patient for accurately recording the relationship between mandible and maxilla and ultimately for controlling the occlusal contact pattern.
The popularity of the concept of CR grew and was soon carried over into the field of fixed prosthodontics. Its usefulness in this context was substantiated both by its reproducibility and early research studies associated with muscle function.12,13
Conclusions from early electromyographic studies suggested that the muscles of mastication function more harmoniously and with less intensity when the condyles are in CR at the time that the teeth are in maximum intercuspation.12–14 For many years the dental profession generally accepted these findings and concluded that CR was a sound physiologic position. More recent understanding of the biomechanics and function of the TMJ, however, have questioned the retruded position of the condyle as the most orthopedically stable position in the fossa.
Today the term centric relation is somewhat confusing since its definition has changed. Whereas earlier definitions11,15 described the condyles as being in their most retruded or posterior positions, more recently16 it has been suggested that the condyles are in their most superior position in the articular fossae. Some clinicians17,18 suggest that none of these definitions of CR indicates the most physiologic position and that the condyles should be ideally positioned downward and forward on the articular eminences. The controversy regarding the most physiologic position of the condyles will continue until conclusive evidence showing that one position is more physiologic than the others is found.
Nevertheless, despite this controversy, dentists must provide needed treatment for their patients. The use of a stable orthopedic position is essential to treatment. It is therefore necessary to examine and evaluate all available information in order to draw intelligent conclusions on which treatment can be based.
In establishing the criteria for the optimal orthopedically stable joint position, the anatomic structures of the TMJ must be closely examined. As previously described, the articular disc is composed of dense fibrous connective tissue devoid of nerves and blood vessels.19 This allows it to withstand heavy forces without damage or the inducement of painful stimuli. The purpose of the disc is to separate, protect, and stabilize the condyle in the mandibular fossa during functional movements. Positional stability of the joint, however, is not determined by the articular disc. As in any other joint, positional stability is determined by the muscles that pull across the joint and prevent dislocation of the articular surfaces. The directional forces of these muscles determine the optimal orthopedically stable joint position. This is an orthopedic principle that is true for all joints. Muscles stabilize joints. Therefore every mobile joint has a musculoskeletally stable position.
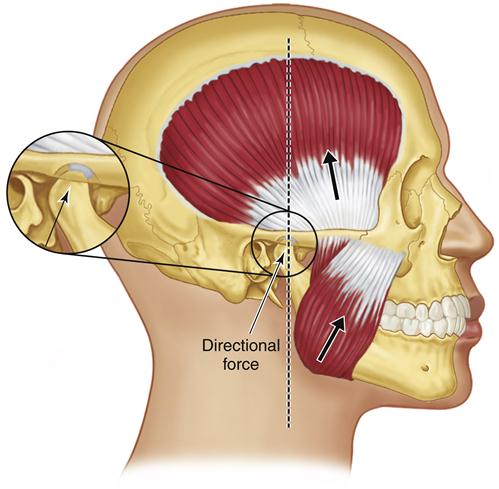
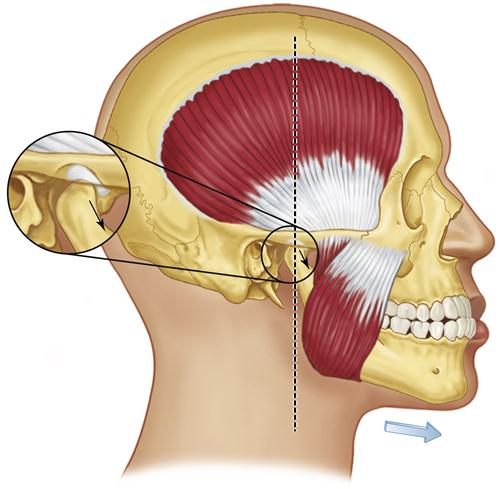
In pursuing the most stable position for the TMJs, the muscles that pull across the joints must be considered. The major muscles that stabilize the TMJs are the elevators. The direction of the force placed on the condyles by the masseters and medial pterygoids is superoanterior (Figure 5-2). Although the temporal muscles have fibers that are oriented posteriorly, they nevertheless predominantly elevate the condyles in a straight superior direction.20 These three muscle groups are primarily responsible for joint position and stability; however, the inferior lateral pterygoids also make a contribution.
In the postural position, without any influence from the occlusal condition, the condyles are stabilized by muscle tonus of the elevators and the inferior lateral pterygoids. The temporal muscles position the condyles superiorly in the fossae. The masseters and medial pterygoids position the condyles superoanteriorly. Tonus in the inferior lateral pterygoids positions the condyles anteriorly against the posterior slopes of the articular eminences.
By way of summary, then, the most orthopedically stable joint position as dictated by the muscles occurs when the condyles are located in their most superoanterior position in the articular fossae, fully seated and resting against the posterior slopes of the articular eminences. The condyles are not down the posterior sloop of the eminences. This movement is certainly possible and represents the functional movement of protrusion. However, this position is not the sound orthopedically stable joint position dedicated by the elevator muscles.
This description is not complete, however, until the position of the articular discs is considered. Optimal joint relationship is achieved only when the articular discs are properly interposed between the condyles and the articular fossae. The position of the discs in the resting joints is influenced by the interarticular pressures, the morphology of the discs themselves, and the tonus in the superior lateral pterygoid muscles. This last causes the discs to be rotated on the condyles as far forward as the discal spaces (determined by interarticular pressure) and the thickness of the posterior border of the discs will allow.
The most orthopedically stable joint position, therefore, exists when the condyles are in their most superoanterior position in the articular fossae, resting against the posterior slopes of the articular with the discs properly interposed. This is the position the condyles assume when of the elevator muscles are activated with no occlusal influences. This position is therefore considered to be the most musculoskeletally stable position of the mandible.
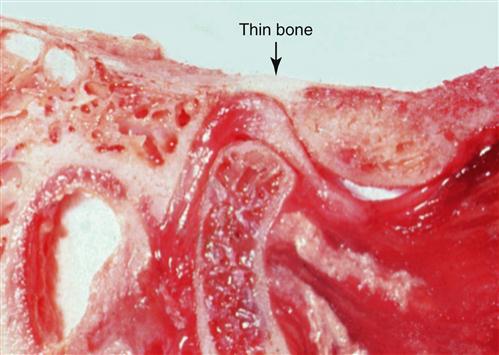
In this musculoskeletally stable (MS) position, the articular surfaces and tissues of the joints are aligned such that forces applied by the musculature do not create any damage. When a dried skull is examined, the anterior and superior roof of the mandibular fossa can be seen to be quite thick and physiologically able to withstand heavy loading forces.19,20 This is also seen in cadaver specimens (Figure 5-3). Therefore, during rest and function the superoanterior position is both anatomically and physiologically sound (see Figure 5-2).
The MS position is now described in the Glossary of Prosthodontic Terms as CR.21 Although earlier definitions9–11 of CR emphasized the most retruded position of the condyles, most clinicians have come to appreciate that seating the condyle in the superoanterior position is far more orthopedically acceptable.
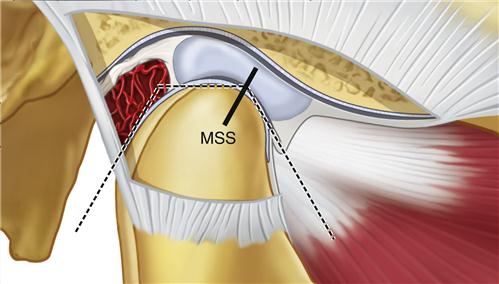
The controversy arises as to whether there is an anteroposterior range in the most superior position of the condyle. Dawson16 suggested that there is not, which implies that if the condyles move either anteriorly or posteriorly from the most superior position, they will also move inferiorly. This may be accurate in the young healthy joint, but all joints are not the same. Posterior force applied to the mandible is resisted in the joint by the inner horizontal fibers of the TM ligament. The most superoposterior position of the condyles is therefore by definition a ligamentous position. If this ligament is tight, there may be very little difference between the most superior retruded position, the most superior position (Dawson’s position), and the superoanterior (MS) position. However, if the TM ligament is loose or elongated, an anteroposterior range of movement can occur while the condyle remains in its most superior position (Figure 5-4). The more posterior the force placed on the mandible, the more elongation of the ligament will occur and the more posterior the condylar position will be. The degree of anteroposterior freedom varies according to the health of the joint structures. A healthy joint appears to permit very little posterior condylar movement from the MS position.22 Unfortunately the health of the joint may be difficult to assess clinically.
Studies of the mandibular chewing cycle demonstrate that in healthy subjects the rotating (working) condyle moves posterior to the intercuspal position during the closing portion of the cycle (Chapter 2). Therefore some degree of condylar movement posterior to the intercuspal position is normal during function. In most joints this movement is very small (1 mm or less). If changes occur in the structures of the joint, however, such as elongation of the TM ligament or joint pathology, the anteroposterior range of movement can be increased. Note that the most superior and posterior (or retruded) position of the condyle is not a physiologically or anatomically sound position (Figure 5-5). In this position, force can be applied to the posterior aspect of the disc, inferior retrodiscal lamina, and retrodiscal tissues. Since the retrodiscal tissues are highly vascularized and well supplied with sensory nerve fibers,23 they are not anatomically structured to accept force. Therefore when force is applied to this area, there is a great potential for eliciting pain and/or causing breakdown.24–28
Once again viewing Figure 5-3, the posterior aspect of the mandibular fossa is seen as quite thin and apparently not meant to bear stress. This feature further emphasizes the fact that the superoposterior condylar position does not appear to be the optimal functional position of the joint.
As discussed in Chapter 1, ligaments do not actively participate in joint function. Their role is to act as limiting structures for certain extended or border joint movements. Nevertheless, for years in dentistry, the use of this border ligamentous position as an optimal functional position for the condyles was discussed. Such a border relationship would not be considered optimal for any other joint. Why would this orthopedic principle be any different for the TMJ?
Since it is sometimes clinically difficult to determine the extracapsular and intracapsular condition of the joint, it is advisable to avoid placing posterior force on the mandible in attempting to locate the musculoskeletally stable position of the joint. The major emphasis should be on guiding or directing the condyles to their most superoanterior positions in the fossae. This can be accomplished either by a bilateral mandibular guiding technique or by the musculature itself (as discussed in later chapters). For the remainder of this text, CR is taken to mean the most superoanterior position of the condyles in the articular fossae with the discs properly interposed. It can thus be seen that CR and the musculoskeletally stable (MS) position are the same. This definition of CR is becoming widely accepted.21
Another concept of mandibular stability18 suggests that a different position is optimal for the condyles. In this concept the condyles are described as being in their optimal position when they are translated to some degree down the posterior slopes of the articular eminences (Figure 5-6). Often this condylar position is determined radiographically; however, owing to angulation and the inability to image the actual articular surfaces of the joint (radiographs image only subarticular bone; see Chapter 9), this technique has not been demonstrated to be reliable. As the condyles are positioned downward and forward, the disc complexes follow; thus forces to the bone are dissipated effectively. Examination of the dried skull reveals that this area of the articular eminence is quite thick and physiologically able to withstand force. Therefore this position, like the most superoanterior position, appears to be anatomically capable of accepting forces. In fact, this is a normal protrusive position of the mandible. The major differences between this position and the MS position lie in muscle function and mandibular stability.
To position the condyles downward and forward on the posterior slopes of the articular eminences, the inferior lateral pterygoid muscles must contract. This is compatible with a protrusive movement. However as soon as the elevator muscles are contracted, the force applied to the condyles by these muscles is in a superior and slightly anterior direction. This directional force will tend to drive the condyles to the superoanterior position as already described (MS). If the maximum intercuspal position were developed in this more forward position, a discrepancy would exist between the most stable occlusal position and the most stable joint position. Therefore, for the patient to open and close in the intercuspal position (which is of course necessary to function), the inferior lateral pterygoid muscles must maintain a contracted state to keep the condyles from up to the most superoanterior positions. This position therefore represents a “muscle stabilized” position, not a “musculoskeletally stable” position. It is logical to assume that this position would require more muscular activity to maintain mandibular stability. Since muscle pain is the most common complaint of patients with masticatory disorders, it would not seem favorable to develop an occl/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


