Chapter 4 Ultraconservative Dentistry
Relevance to Esthetic Dentistry
The establishment of porcelain veneer techniques as a basic treatment modality has been a rapid and welcome development (Figure 4-1). Many dentists offer this procedure as a routine service to their patients. In the continuing effort to deliver predictable, high-quality restorations, the dentist must be aware of the interplay between dental tissues and restorative materials (Figure 4-2). Today’s patients are more involved and more knowledgeable, more keenly aware of their bodies, and less likely to accept invasive procedures than patients just a few years ago. Esthetic concerns are still very important, but not at the expense of tissue integrity. When porcelain veneers were introduced, one of the major underlying advantages was the conservative nature of the procedure. The minimal preparation advocated represented a significant advance over full-crown preparation techniques. Since then many practitioners have found it easier to correct color and shape by removing a 0.5-mm (or greater) thickness of healthy tooth structure, subsequently replacing natural tooth structure with opaques, bonding agents, and porcelain. The ultraconservative technique for porcelain veneers, involving minimal tooth structure removal, is respectful of healthy dental tissues and highly esthetic, making it potentially beneficial to both patient and dentist.


Brief History of Clinical Development and Evolution of the Procedure
Dental ceramics have long been recognized for their similarity to dental enamel (Figure 4-3). They can be made to closely mimic the shades and textures of the natural tooth. Porcelain provides the practitioner with the clinical ability to restore a patient’s dentition to its original appearance and function.

Over the past two decades the use of bonded porcelain has expanded exponentially. Previously, the weak link in ceramic procedures was the cement used to affix the restoration to the prepared tooth. Zinc oxyphosphate (Figure 4-4, A) cement and similar luting agents (Figure 4-4, B) were intended to simply occupy the space between the tooth and the crown that was inadvertently created during the manufacturing of the restoration. These materials did not impart any chemical or physical integration to the overall restorative treatment process.
FIGURE 4-4 A, Zinc oxyphosphate cement. B, Polycarboxylate cement.
(Courtesy Shofu Dental Corporation, San Marcos, California.)
The more recent composite resin cements not only take up the spaces that exist between the crown and abutment but also integrate the restoration and the tooth both micromechanically and chemically (Figure 4-5). As a result, all the components—tooth, resin cement, and restoration—act as a unit structure, or monobloc. Contributing to this trend are increased patient involvement in the dentistry process, better education, intraoral cameras, and a heightened sense of esthetics. Increased patient awareness has led to more active involvement by patients in selecting their own treatment modalities. Patients are less likely to readily accept invasive procedures. Although esthetics is a major motivator, to many the integrity of healthy tissue is paramount. The dentist is thus faced with the task of integrating the patient’s dental needs with treatment options that are maximally conservative of healthy tooth structures and respectful of periodontal tissues while being highly esthetic. The dental armamentarium today offers both the techniques and the materials to accomplish these goals.

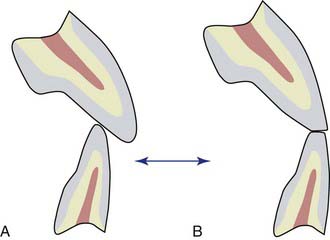
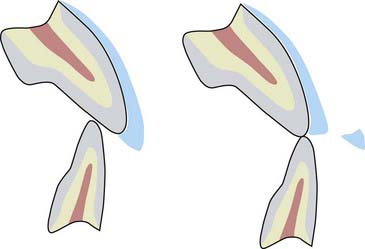
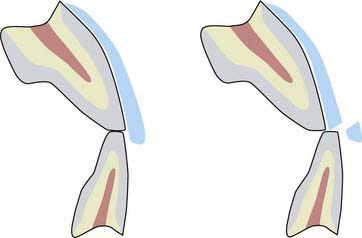
Rehabilitation of the dentition has been extensively described in the dental literature. Before currently available techniques and materials, these procedures routinely required aggressive preparation of all the teeth involved—not a tissue-conservative approach (Figure 4-6). This approach occasionally led to the extensive use of preprosthetic elective endodontic treatment because the remaining natural teeth demonstrated nonparallel angulation (Figure 4-7). Often, complex periodontal treatment was required to reestablish a stable soft tissue environment. These procedures could take months or years to complete, causing stress for both patient and dentist. Many patients, faced with a realistic description of the required treatment, declined to proceed. With the application of newer materials and techniques, minimally invasive, or ultraconservative, approaches have been developed to address these dental problems. Ultraconservative dentistry is respectful of the soft tissues, seeks to minimize the removal of healthy tooth structure, is highly esthetic, and uses the strengths of restorative materials to reinforce the remaining dentition.


Relating Function and Esthetics
Occlusal Vertical Dimension
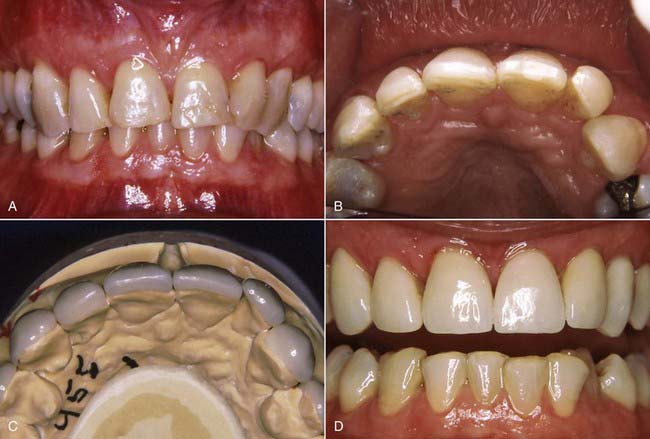
The posterior dental support present in the young (or ideal) occlusion can be lost to age, wear, function, fracture, and parafunction. The loss of posterior masticatory support can eventually cause excessive wear on the anterior teeth (Figure 4-8, A and B). The resulting flat or even smile line (Figure 4-8, C) is often associated with an older appearance, regardless of the patient’s chronologic age. This is generally viewed as an undesirable esthetic condition, and many patients prefer a more youthful smile (Figure 4-8, D).

An established method for treating this situation is the use of bonded porcelain veneers. Although veneers can be made long enough to make the resulting gingivo-incisal appearance acceptable, there may not be enough anterior interocclusal space to accommodate all the ceramic that is required for esthetics (Figure 4-9). A long unsupported incisal extension of ceramic veneers tends to interfere with the opposing incisors, causing extensive wear, fracturing, or both (Figure 4-10). One way to create adequate vertical extension space for worn anterior teeth is to recreate the posterior occlusal vertical dimension. In recent decades, posterior teeth have been more likely to be worn than missing, a result of the improved dental education and oral hygiene of the population in general.
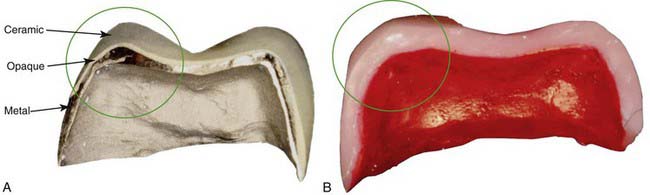
When selecting the most conservative approach to restore these posterior teeth to their original (or ideal) occlusal vertical dimension, a bonded, all-ceramic onlay restoration best fits the required parameters (Figure 4-11). A ceramometal restoration has three components (metal, opaque, and ceramic) (Figure 4-12) and requires a prescribed thickness and thus greater tooth removal for each layer. An all-ceramic onlay (Figure 4-13) eliminates two of these layers—the metal and the opaque—and thus requires less thickness and consequently less removal of healthy tooth structure. Furthermore, the ceramic bond to tooth structure is stronger and more predictable than the bond of metal to tooth.
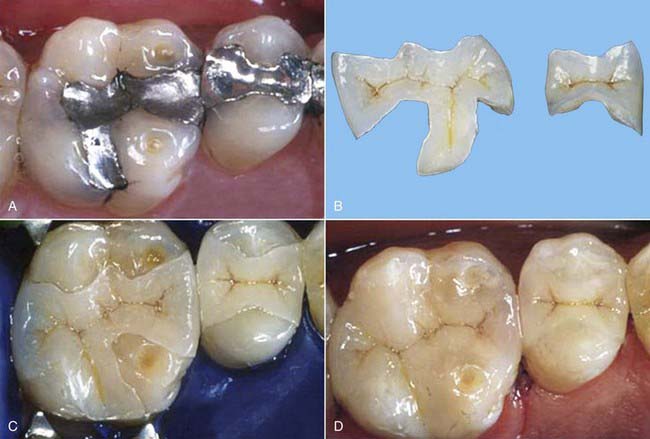
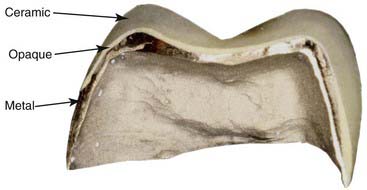
FIGURE 4-12 Cross-section of the ceramometal restoration shows three components—metal, opaque, and ceramic.
Several methods are used to develop and alter the patient’s occlusal vertical dimension (Figure 4-14, A). Ultimately, the patient’s function is the best guarantor of long-term stability. Through use of established guidelines for determining the vertical opening in complete denture patients, an initial interdental opening is estimated. An occlusal bite plate (Figure 4-14, B) is made that maintains this opening over a length of time to gauge the patient’s comfort with the altered occlusal vertical dimension (Figure 4-14, C). The bite plate can be adjusted as required until the patient is completely comfortable. Typically, bite plates are white or translucent; for demonstration purposes, in the figure it is a strong orange color.


Once the altered occlusal vertical dimension has been well tolerated for several weeks or months, depending on the age and oral condition of the patient, the final restorations that open the bite to the new position may be fabricated. Adding to the occlusal vertical dimension typically increases the anterior facial height, further enhancing the youthful appearance imparted by this dental procedure (Figure 4-14, D to G).
Clinical Considerations
Considerations in Ultraconservative Veneer Preparation
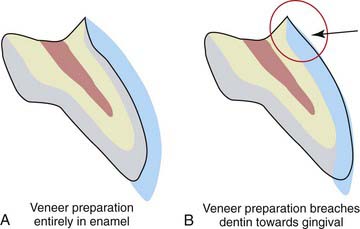
The primary concern is for healthy tooth structure. In the interest of maximizing bond strength, all the buccal enamel should be retained (Figure 4-15). Where some minimal preparation is necessary, however, the preparation must be left in the enamel layer if at all possible.
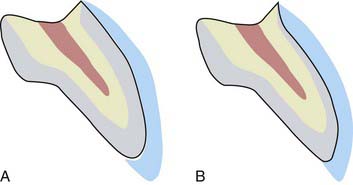
FIGURE 4-15 A, All the buccal enamel has been retained. B, Preparation for the veneer kept within enamel.
Almost any preparation, no matter how shallow, penetrates to the dentin at some point, usually toward the gingival portion of the tooth (Figure 4-16), where the enamel thickness flares down to a knife edge at the cemento-enamel junction. In the earlier days of porcelain veneers, only enamel bonding agents were available for securing laminates. Thus the area most prone to leakage (resulting in veneer failure) was the margin that terminated in dentin. The initial signs of subveneer staining were followed by percolation, then fracture of the gingival segment of the laminate (Figure 4-17). Even with the best of the newer dentin adhesive agents, the porcelain bond to enamel is still significantly greater than the adhesion to dentin, so it is advisable to minimize dentin exposure during preparation.

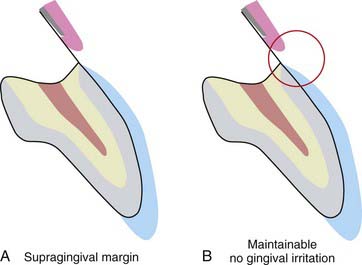
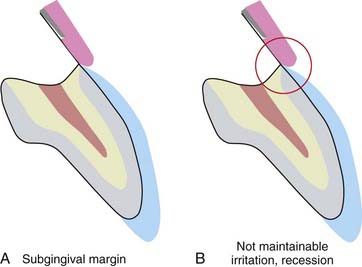
The margins of the porcelain veneer should be placed where the patient can readily access them for routine home maintenance. In particular, the gingival margin should be located supragingivally (Figure 4-18). The microenvironment of the veneer margin consists of a knife-edge silanated porcelain bonded onto enamel by a composite resin cement. The enamel and porcelain are both biocompatible with the gingiva and well tolerated. The composite, however, tends to cause irritation if it comes into intimate contact with the gingiva. When the margin is placed subgingivally, this luting material is in direct contact with the free gingival margin, eventually causing irritation and recession (Figure 4-19). With a supragingivally margined veneer, the composite is reasonably away from periodontal structures and is unlikely to cause tissue irritation.
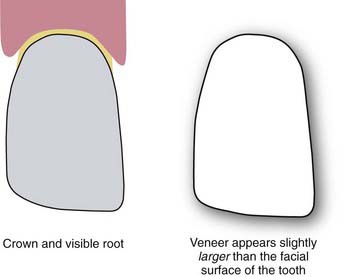
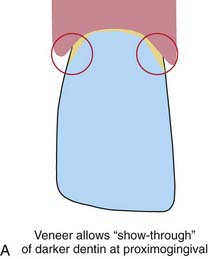
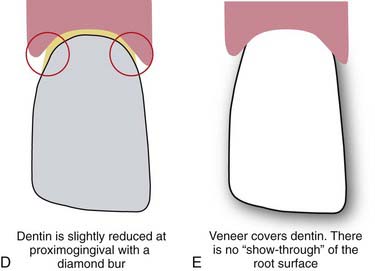
All visually accessible areas of the tooth should be covered by porcelain (Figure 4-20). The area most often overlooked in this respect is the gingival portion of the proximofacial line angle (Figure 4-21). With gingival recession, these areas of slight concavity are uncovered. The dark underlying tooth structure is visibly unesthetic when the patient is viewed from the side. A slight reduction of the proximofacial line angle is usually all that is needed to permit an acceptable path of insertion for the proximally extended porcelain laminate (Figure 4-22).


Indications
Ultraconservative dentistry usually involves several approaches. Rather than removing excessive tooth structure in order to create room for a veneer, veneers are placed with little or no surface preparation if possible. This is the ideal situation, but it may not always be achievable (Figure 4-23).
For posterior onlays, when the occlusal vertical dimension is to be opened, if the occlusal surface is intact and healthy, or restored with composite or ceramic, an onlay can be bonded onto the existing tooth surface, simply extending its vertical height, without necessarily preparing the tooth surface (Figure 4-24). This qualifies as ultraconservative dentistry. Minimal preparation is part of ultraconservative dentistry, but the ideal is always no preparation at all.
Material Options
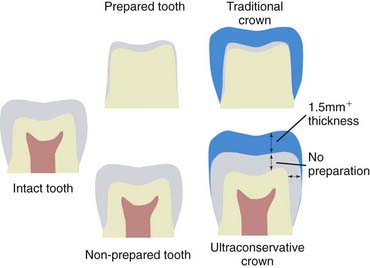
The crown and bridge metals used in dentistry are effective, but they require more extensive preparation of tooth structure to develop physical retention and/or leave space for the ceramic that can completely hide the color of the metal. In comparing a ceramic restoration with a porcelain-fused-to-metal restoration, the ceramic restoration must cover, change, or maintain the color of the underlying abutment. The porcelain-fused-to-metal restoration, on the other hand, is adapted to the underlying tooth structure, but then requires opaquers to hide the color of the metal and subsequently various layers and thicknesses of ceramics to hide the underlying color of both the metal and the opaquers to create a natural-looking, esthetic tooth. Thus the porcelain-fused-to-metal restoration tends to be much thicker than its all-ceramic or composite counterpart and is inherently less conservative than restorations accomplished with these materials (Figure 4-25). In addition, metals generally do not bond to tooth structure, enamel, and dentin as well as the composite and ceramic materials.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


