4
4
Orthodontic Preparation
Timing and Duration
The objectives of presurgical orthodontic treatment are to enable maximal surgical correction of the deformity, to facilitate any segmental surgical procedures and to enable the production of an ideal stable occlusion. An essential feature of the treatment plan is to decompensate the dento-alveolar results of the jaw deformity and as such is very different from the “compensatory” approach of the pure orthodontic management of the case. Hence the need for careful consideration by the patient and clinicians as to the desired choice of treatment. The majority of orthodontic treatment is undertaken prior to surgery, although some prefer to undertake minimal orthodontic treatment prior to surgery leaving the major proportion to the postoperative phase. Both of these approaches have advantages and disadvantages. Extensive presurgical preparation is usually better accepted by the patient giving maximum compliance. However, the dental movements may be hindered by the underlying skeletal and soft tissue discrepancy. Conversely, although the orthodontic changes may be easier once a normal skeletal and soft tissue relationship has become established, prolonged postoperative orthodontics may not be tolerated by the patient and leads to poor patient satisfaction.
Presurgical Orthodontics
Presurgical preparation usually takes 18-24 months, whilst postsurgical refinement should be completed within 6 months of the operation.
The goals of presurgical orthodontics are to facilitate the surgery by:
- Alignment of the dentition.
- Levelling of the occlusal plane, either as a continuous arch or segmentally prior to surgical levelling.
- Incisor decompensation.
- Buccal segment decompensation.
- Coordination of the upper and lower arches.
- Providing a means of fixation.
Alignment of the Dentition — The Technology
Dental arch alignment requires 3-dimensional control of tooth position. Most use a pre-adjusted Edgewise appliance system with a slot dimension of .022” × .028” or variants upon this. The term preadjusted appliance refers to the bracket design such that adjustments are incorporated into the brackets to create a final position of the teeth with the correct mesiodistal angulation (tip), buccopalatal or buccolingual inclination (torque) and horizontal positions (in/out) relative to each other. Individual teeth within the dental arch therefore have specific adjustments built into their appropriate bracket (Figure 4.1). A variety of pre-adjusted systems are available each with minor variations in the tip and torque values. This is referred to as the bracket prescription. Segmental surgery requires the added facility of a double tube on the mandibular molars and/or a triple tube on the maxillary molars. The Tip-EdgeTM appliance system is equally applicable to presurgical alignment although individual operators will have their preferred bracket prescription.
It is worthwhile considering the variations in bracket tip and torque required in specific cases. In an ideal occlusion, the crown of the lower incisor lies labial to the apex for ideal tooth inclination. In Class II cases where proclined lower incisor require decompensation, the use of MBTTM brackets with the 60 of additional lingual crown torque can aid the mechanics. Conversely, Super-torqueTMbrackets, with additional palatal root torque to the upper incisors, can be useful in correcting severely retroclined incisors in Class II division 2 cases. Mesiodistal tooth angulation (tip) becomes important when considering the preparation of a case for segmental surgery as it is important to facilitate the surgery (see below) by ensuring the roots adjacent to the osteotomy site are either parallel or slightly divergent. Again in an ideal functioning occlusion, the crown of the canine should lie mesial to the apex. Where the osteotomy cuts are to be made distal to the canines, the use of the canine bracket of the opposite side ensures that the tip incorporated into the bracket keeps the apices forward and out of the way of the surgical cuts.
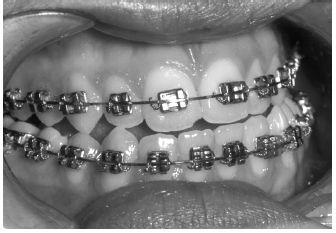
Figure 4.1 Pre-adjusted Edgewise appliances with individual brackets designed for specific teeth.
The choice of archwire material and sequence is to a large extent, driven by operator preference. The use of modern “superelastic” nickel titanium wires is frequently beneficial for initial alignment. However, where the interbracket span is minimal, for example with mutually rotated lower incisors or premolars, the efficiency of these wires is reduced. In this situation, archwires with loops for flexibility may be preferable, for example .014” or .016” stainless steel or Titanium/Molybdenum (TMA) wires. Ultimately, heavy rectangular stainless steel archwires should be placed at the time of surgery (.019” × .028” or .022” × .028”) for maximal tooth control and with the addition of hooks to facilitate fixation.
Arch Levelling
The decision as to whether to fully level the arches is very much dependent on the patient’s facial height and the upper lip/incisor relationship. In Class II corrections, where the facial height is reduced, it is preferable to preserve a Curve of Spee in the lower arch so that when the mandible is advanced, the lower incisors slide down the cingulum plateau of the upper incisors thereby increasing the lower facial height (Figure 4.2). Although this may occur in some Class II division 1 cases, it is especially common in patients with Class II division 2 incisor relationships where the presurgical orthodontic preparation converts the incisors into a Class II division 1 pattern.
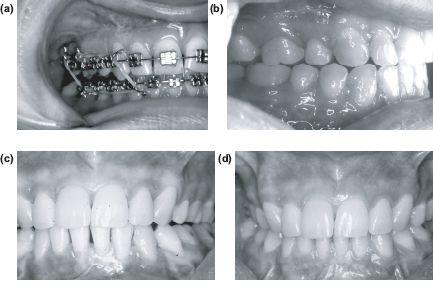
Following surgery this results in buccal segment lateral open bites with occlusal contact in only the incisor and terminal molar regions. This tripod of contacts is referred to as a “3-point landing”. The lateral open bites (Figure 4.3) require closure as part of the postsurgical orthodontic phase of treatment (see Chapter 10).
In Class II cases where the intention is to avoid increasing the facial height, the lower arch should be levelled as part of the presurgical orthodontic preparation, or by segmental surgical procedures. With a shallow curve of Spee (approximately 2 mm), it may be possible to level the arches orthodontically through a combination of buccal segment extrusion, incisor intrusion and/or incisor proclination (Figure 4.4). Levelling the Curve of Spee without space will procline the lower incisors, and reduce the potential for mandibular advancement. If the intention is to maintain anteroposterior arch length, then premolar extractions will be required, especially if there is any crowding present (Figure 4.5).
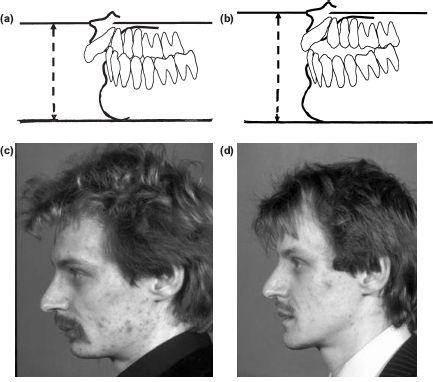
Figure 4.2 (a) and (c) Class II deep overbite cases, with an increased curve of Spee, facilitates an increase in anterior face height as the mandible is advanced (b) and (d). The resulting contact between the upper and lower incisors and the terminal molars of each side of the arch is referred to as a “3-point landing”. Note the significant increase in lower facial height accompanying the advancement.
Segmental Levelling
a) In cases of reduced vertical dimension
In cases with a severe overbite the so-called “3-point landing” may produce lateral open bites which are too large to close by orthodontic extrusion of the premolars and canines. Many operators consider 2 mm of extrusion from each arch as the absolute maximum that can be achieved and remain stable without rebound. Beyond this, levelling should be achieved through surgery, usually through a set-down of the lower labial segment with a mandibulotomy (see Chapter 9). Where there is a reverse Curve of Spee in the upper arch, as in some Class II division 2 cases, it may be necessary to undertake segmental surgery to both the upper and lower labial segments.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


