Chapter 4
Clinical Examination and Local Risk Factors for Periodontal Diseases
Aims
This chapter outlines the key stages of the initial periodontal examination for children, adolescents and young adults and describes local risk factors for the periodontal diseases relevant to this age group.
Outcome
Having read this chapter, the practitioner should understand the key stages of the periodontal examination of children, adolescents and young adults and be able to identify local periodontal risk factors pertinent to these patients. They should also appreciate the role of the Basic Periodontal Examination (BPE) in screening young adults and be familiar with the use of a simplified form of the BPE for children and adolescents. In addition, the reader will also be familiar with current regulations and guidance for the use of radiographs in young patients with periodontal diseases.
Examining Children, Adolescents and Young Adults
The routine dental examination (Fig 4-1a) of children, adolescents and young adults should include the following:
-
Extraoral examination
-
Intraoral examination (Fig 4-1b):
-
soft tissue examination
-
dental charting of teeth present, restorations, cavities, etc.
-
general description of periodontal condition, to include:
-
gingival colour
-
gingival contour
-
presence of swelling
-
presence and location of inflammation
-
presence of gingival recession
-
presence of suppuration
-
qualitative assessment of oral hygiene and presence of supragingival calculus deposits
-
occlusal problems, drifting/tooth migration and related aesthetic problems.
-
-
identification of local periodontal risk factors
-
screening using BPE
-
special tests:
-
radiographs
-
vitality tests.
-
-
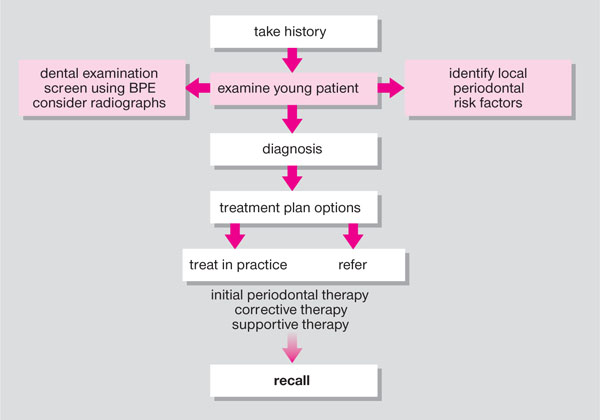
Fig 4-1a Stages in periodontal patient management: examination.
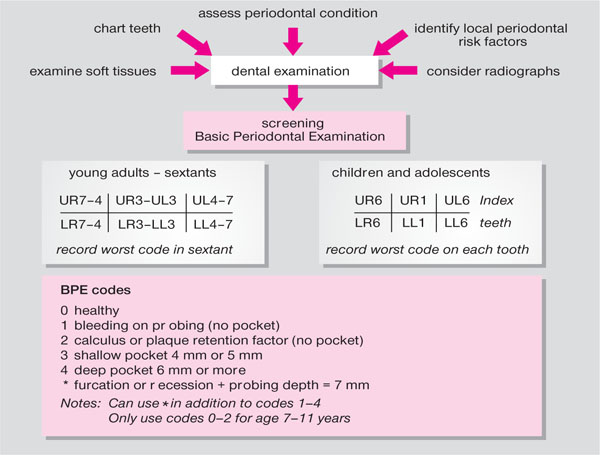
Fig 4-1b Dental examination and periodontal screening using the Basic Periodontal Examination (BPE) for children, adolescents and young adults.
The general principles and details of the examination are described in the first book of this series (see Chapple and Gilbert 2002), therefore the present account will focus on the key aspects of local factors, screening and radiographs that pertain to the younger age groups.
Local Risk Factors
Local risk factors can increase the risk of periodontal disease development and progression principally by acting as plaque retention factors. These factors should be investigated during a thorough dental examination of the patient (Box 4-1).
Box 4-1
Local Risk Factors for Periodontal Diseases
Calculus (supra- and subgingival)
Restorations
Fraenal attachments
Orthodontic appliances
Malocclusion or crowding/imbrication
Local trauma
Mouth breathing and lack of lip seal
Xerostomia
Anatomical features
Calculus
Supra- and subgingival calculus deposits act as local plaque retention factors. Although calculus deposits are expected in adults, subgingival calculus is also common in teenagers. It has been shown that subgingival calculus is related to gingival inflammation and attachment loss in adolescents (Fig 4-2). A relationship has also been found between ethnicity and subgingival calculus deposits in adolescents with deposits more prevalent in young Asian patients.
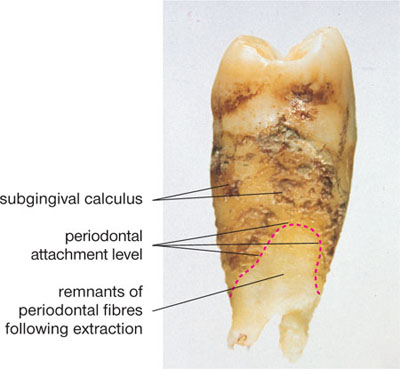
Fig 4-2 Subgingival calculus in association with loss of attachment on extracted tooth.
Restorations
Subgingival restoration margins, marginal discrepancies and overhanging restorations have all been associated with gingivitis and attachment loss due to the difficulties they present for plaque removal – not for direct irritation of the tissues. In Western countries there has been a trend towards improved child dental health over the past decade. With further caries prevention measures, there should be fewer restorations impacting on the gingival tissues. Nevertheless, dental caries is still a common condition, particularly in areas of social deprivation. Sites with extensive proximal caries have been associated with bone loss and restoration of such sites has been associated with bony infill. The use of matrix bands, wedges, the adaptation of stainless steel crown margins and careful clinical and laboratory techniques for the provision of cast restorations will help to produce restorations in the young patient that should not have any future periodontal consequences.
Fraenal Attachment
A prominent fraenum can act as a local plaque retention factor by impeding access to the toothbrush (Fig 4-3a and b). Direct fraenal pull has been described as an aetiological factor in gingival recession, but this is unlikely to be a common contributing factor.

Fig 4-3 (a,b) High fraenal attachments impeding tooth brushing. (b) Note plaque deposits in association with localised gingival recession in 11-year-girl.
Orthodontic Appliances
Fixed and removable orthodontic appliances are commonly worn by children and adolescents and considerable effort is required by the patient to maintain a clean mouth (Fig 4-4). Some young adults wear orthodontic appliances for the alignment of teeth that have drifted due to periodontal disease once the disease has stabilised following periodontal therapy. Important issues to consider include:
-
access to interdental cleaning is diminished and plaque is more likely to accumulate
-
gingivitis commonly occurs after placement of fixed orthodontic appliances and enamel decalcification can occur around bonded attachments
-
teeth with bands are harder to access for cleaning and bands extending to the gingival tissues increase the likelihood of plaque retention and gingivitis
-
if oral hygiene is good then the deleterious effects are minimal
-
coronal attachment loss can occur during orthodontic appliance therapy and can range from an annual loss of 0.05–0.3mm
-
apical root resorption is also a common consequence of orthodontic treatment that results in a reduced length of root (Fig 4-5) supported by bone even though no coronal (plaque-induced) alveolar bone loss has occurred in these circumstances
-
direct trauma from components of orthodontic appliances can cause local injury to the soft tissues
-
chronic trauma may lead to gingival overgrowth or a fibrous epulis may develop (Fig 4-6)
-
if teeth are orthodontically moved within alveolar bone there is generally little risk of soft tissue recession
-
orthodontic tooth movements associated with excessive proclination of lower incisors and arch expansion do carry an increased risk of gingival recession. It is important to anticipate this scenario and consider a preorthodontic connective tissue graft to provide a keratinised labial gingiva (Fig 4-7a,b)

Fig 4-4 Plaque around fixed orthodontic appliance, disclosed in the lower arch to aid visibility.
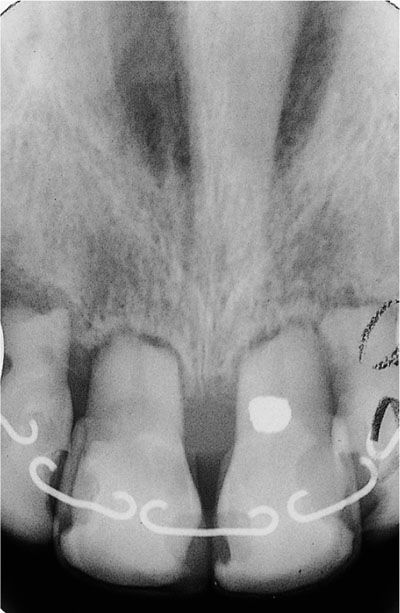
Fig 4-5 Apical root resorption following orthodontic treatment.

Fig 4-6 Fibrous epulis related to chronic irritation from subgingival calculus acting as a plaque retention factor.

Fig 4-7 (a,b) Pre-orthodontic connective tissue graft to provide keratinised labial gingiva; (a) pre-graft, (b) post-graft surgery.
Malocclusion
An association between irregularity of teeth and gingivitis has been demonstrated. Oral hygiene measures are harder to implement at sites where teeth are imbricated, rotated, markedly retroclined or proclined. However a lack of orthodontic treatment does not seem to have much effect on periodontal diseases later in life. A severe overbite can cause direct trauma to the upper palatal or lower labial gingival tissues which may be associated with gingival recession.
Local Trauma
Direct local trauma can be the result of habits such as an aggressive t/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


