36
Preparation for Porcelain Laminate Veneers
Porcelain laminate veneers (PLVs) have proved to be one of the most successful and long-lasting indirect aesthetic restorations. However, PLVs are also one of the most clinically and technically challenging restorations, and their success is attributed to careful and meticulous protocols. PLVs are the most frequently used and abused restorations in cosmetic dentistry, especially in the case of ‘extreme make-overs’. In addition, careful analysis of the patient’s psyche is essential before embarking on irreversible elective cosmetic procedures, particularly if expectations are beyond clinical feasibility.
Rationale
The ethos of PLV is based on the principles of preserving as much natural tooth substrate as possible, especially enamel, and utilising this natural hard tissue foundation to support thin veneers of porcelain. Generally, resin-bonded PLVs require 1/4 to 1/2 tooth reduction compared to complete coverage crowns. In addition, PLVs conserve natural tooth structure, tooth vitality, rigidity and structural integrity, prevent postoperative sensitivity and therefore ensure longevity of both the tooth and veneering porcelain.
To prevent mutilation of tooth structure for spurious short-term aesthetic gains, it is worth remembering the following dictum before prescribing PLV:
The purpose of PLV is replacing lost enamel and dentine
not
As a substitute for enamel and dentine
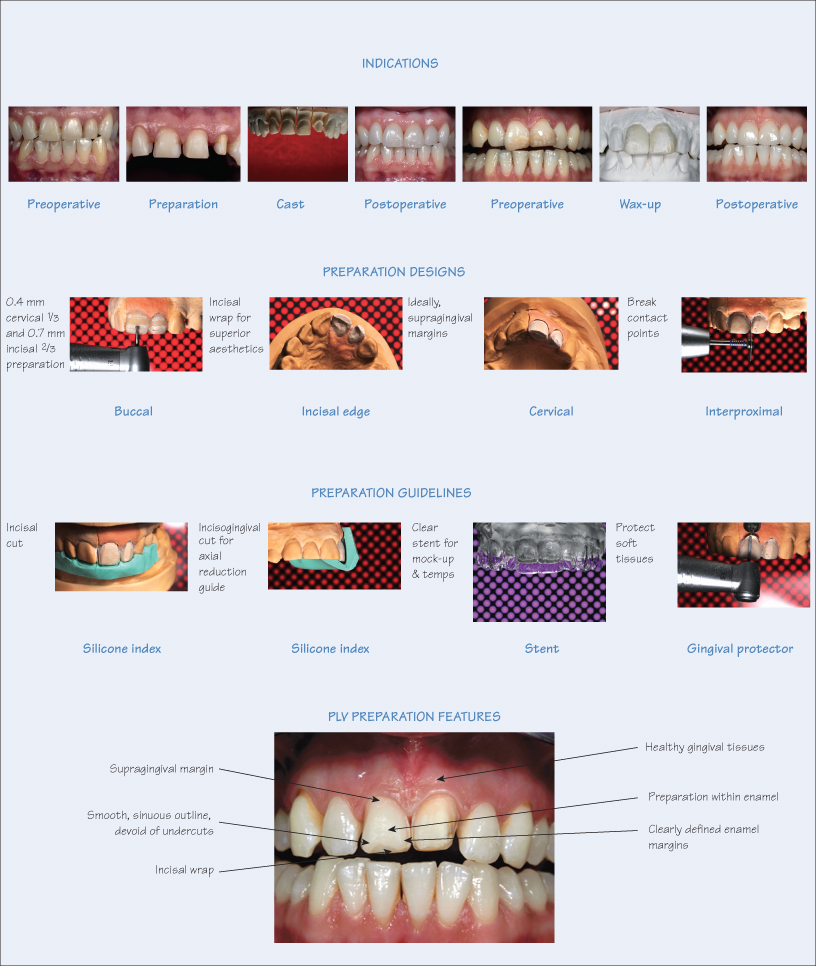
Indications for Porcelain Laminate Veneers
PLVs are primarily aesthetic restorations for improving tooth colour, morphology and alignment. They are usually placed on buccal surfaces of teeth in the maxillary anterior sextant, but are also indicated for:
- Space management, e.g. diastemata closure, or correcting imbrications;
- Restitution of occlusal vertical dimension (OVD) using the
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


