CHAPTER 3
Investigations
Radiographs
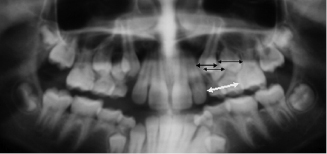
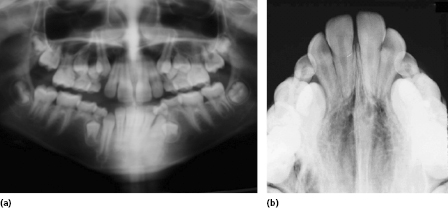
The orthopantogram (OPG) and anterior occlusal radiographs are the X-rays of choice for an orthodontic examination, and allow for the assessment of the presence of teeth, their position, the degree of crowding and any bone pathology, as well as the basic quality of the dentition and of restorations (Figure 3.1). Early assessment is important as often ectopically positioned teeth or hypodontia can be managed by the early extraction of primary teeth. The position of the maxillary canines is particularly unpredictable and can be identified in three planes of space by using vertical parallax with OPG and upper anterior occlusal radiographs. Parallax employs the tube shift method of radiographic localisation of objects: an object that is near to the source of the X-rays will move in the opposite direction to the shift in the X-ray tube and those further away will move in the same direction. An OPG is fixed in the horizontal plane and the anterior occlusal radiograph is at roughly 60° to the horizontal and requires a ‘shift’ in the tube position. By comparing an unerupted tooth to the root of an adjacent tooth, its bucco-palatal position can be accurately determined (Figure 3.2).
Assessing Crowding on OPG Radiographs
This method of assessing crowding has the advantage of being able to predict at an early stage whether extractions will be necessary as part of comprehensive orthodontic treatment. Although there is often distortion on a tomograph, although the image of the posterior segments is usually easily visualised and gross measurements can be easily made. By measuring the mesio-distal widths of the canines and premolars and the distance between the distal edge of the lateral incisor and the mesial edge of the first molar, a reasonable assessment of the dento-alveolar disproportion can be made. Obviously, as the dentition erupts, there will be considerable further growth and development, but these measurements give a very good indication if extractions are necessary. Where there is significant crowding, early extraction of a premolar unit will allow space for the eruption of a canine and second premolar unit into the line of the dental arch without becoming ectopic. This will shorten the orthodontic treatment or even eliminate the need for it. If the crowding is assessed to be mild, the clinician will have additional justification for early arch expansion if there is an asymmetric maxillary arch or crossbite.
Cephalometric Evaluation
A lateral cephalograph can be used to assess the jaw position, to monitor craniofacial growth and mandibular rotations, and to identify changes with treatment (Figure 3.2). Cephalometric evaluation provides numeric data to identify skeletal and dental discrepancies; however, it must be remembered that this evaluation only supports the clinical diagnosis and that numeric data do not always translate into good aesthetics. Great care has to be taken during treatment planning not to give undue importance to specific angles and distances measured on these radiographs, as overall facial aesthetics is the primary goal (Figure 3.3).
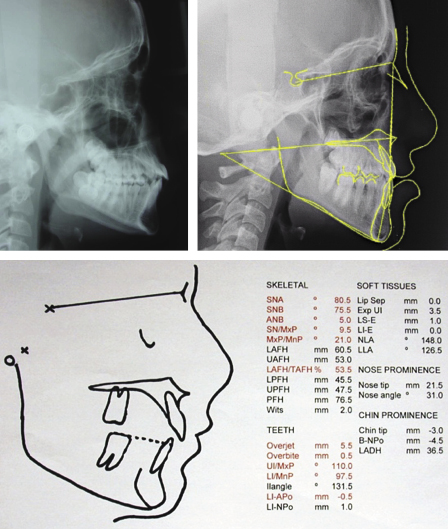
If a cephalometric assessment indicates the upper incisors are inclined beyond the expected normal value for that individual, this does not mean that the teeth are proclined in the face or that they are unstable. It is possible that the maxilla is positioned such that the incisors are aesthetically pleasing even at this increased angulation. However, treatment changes (the changes in tooth inclination with appliances) can be reasonably accurately assessed using measurements taken from a lateral cephalograph. The relationship of the skeletal bases can be assessed from the severity of the discrepancy between the upper and lower jaws. Once this has been determined, the amount of dento-alveolar change needed to satisfy the patient’s wishes and to ensure reasonable post-treatment tooth position can be assessed. The stability of the tooth position after orthodontic treatment is uncertain and depends not only on growth but also on soft tissue balance as well as the initial tooth displacement. Current thinking is that the stability of the tooth position cannot be guaranteed as the soft tissue ‘neutral zone’ in which the teeth sit (with the tongue pushing out and the lips and cheeks pushing in) together with the effect of the periodontal and supragingival fibres change with maturity. Whether the neutral zone is wide or narrow, it cannot be predicted whether this width will change over time and therefore stability of individual teeth after orthodontic tooth movement can only be guaranteed by using retainers. The amount of time retainers need to be worn, both in terms of hours per day and for how many months or years, is always subjective and will be different for each individual patient. The decision must be made by considering both the initial malocclusion and the amount of tooth movement to be achieved during treatment. Cephalometric analysis should never be used to predict stability.
Cone-Beam Computed Tomography
Cone-beam computed tomography (CBCT) is a fast developing technology that provides relatively low-dose, high spatial resolution imaging of the craniofacial complex in three dimensions (3D) (De Vos et al., 2009). It is increasingly being utilised in orthodontics, oral and maxillofacial surgery, implantology and restorative dentistry. CBCT has proven especially useful for the location of pathology and delineation of structures, but care has to be taken as the detailed information gained from 3D imaging can expose our limitations in interpreting the findings. Identification of pathology that is not routinely seen on 2D images can lead to confusion or clinical error if clinicians are unable to interpret or manage the findings because of the limited evidence base.
CBCT utilises a cone-shaped X-ray beam, which rotates synchronously around the patient’s head with an area detector. This captures an entire region of interest in a single rotation of the radiation source, unlike the ‘multiple slices’ that are generated by conventional CT (Kau et al., 2005). CBCT output gives a cylindrically shaped volume of the patient’s bony skeleton. The volumetric data set contained in this ‘cylinder’ consists of a 3D block of cuboid structures, known as voxels. Each voxel represents a specific degree of X-ray beam absorption. Image reconstruction is achieved using computer software programs that utilise sophisticated algorithms and reconstructing the images in three orthogonal planes; sagittal, coronal and axial.
CBCT is an effective imaging technology producing dimensionally accurate information, with small volume scanners offering lower radiation doses and good image quality. At present, and in keeping with the latest recommended guidelines (Ionising Radiation Medical Exposure Regulations 2000), the use of CBCT is only appropriate in select cases where conventional radiography has failed to provide adequate diagnostic information (Arai et al., 1999). A number of areas where CBCT is useful are described here. Others that are outside the scope of this book include planning for temporary anchorage devices, rapid maxillary expansion, cleft palate and orthognathic surgery.
Detection of Impacted/Ectopic Teeth
Current mainstream practice for the localisation of impacted teeth involves 2D radiographic imaging using conventional radiographs, such as dental panoramic tomograms (OPGs) and periapical views, which provide information about the vertical and mesio-distal relationships of the unerupted tooth with neighbouring teeth and roots. These radiographs may be supplemented with other 2D images, such as occlusal radiographs and lateral cephalograms. However, plain film 2D imaging may not be sufficient for the identification of structures because of distortion, magnification and imaging artefac/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


