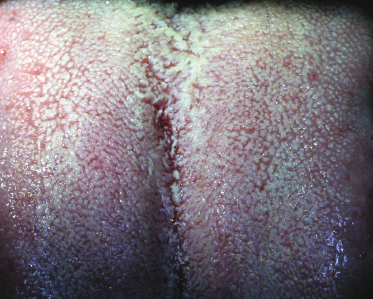
White coated tongue (Fig. 3.1) Figure 3.1 Common white coating of the dorsal tongue.
Site—tongue dorsum.
Morphology—thin film or plaque from sloughing keratin.
Color—white.
Signs and symptoms—can be scraped off with difficulty. Some diffuse lesions cannot be scraped off.
Treatment—brush tongue daily to minimize accumulation of bacterial debris and keratinized slough.
Candidiasis
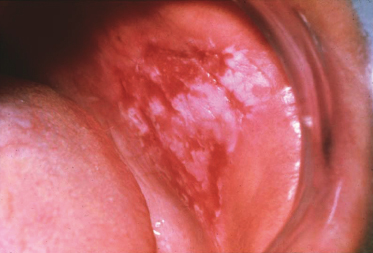
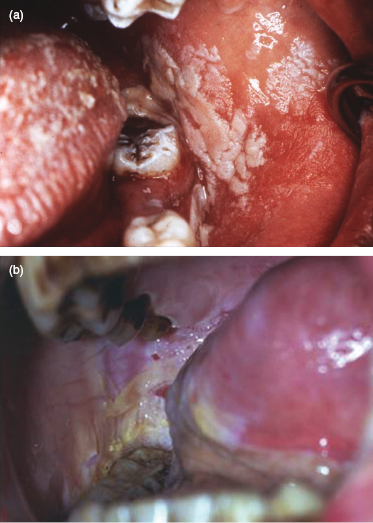
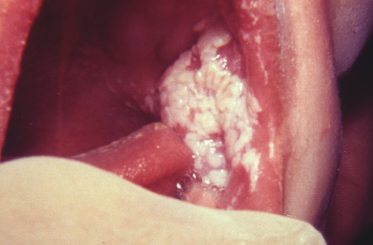
Acute pseudomembranous type (also called thrush) (Fig. 3.2) Figure 3.2 Acute pseudomembranous candidiasis of the buccal mucosa with a portion removed, revealing a red underlying base.
Site—buccal mucosa, palate, and dorsal tongue are most common.
Morphology—plaques composed of tangled masses of hyphae, yeasts, desquamated epithelial cells, and debris.
Color—creamy-white.
Signs and symptoms—resembles cottage cheese or curdled milk; can be scraped or rubbed off with dry gauze, leaving an underlying pink or red mucosa. There may be no symptoms or a mild burning sensation or an unpleasant “salty” or “bitter” taste. Thrush can be initiated by impairment of the immune system or by broad-spectrum antibiotics, which eliminate competing bacteria.
Treatment—prescription antifungal agents: cream, ointment, liquid, and tablets.
Chronic hyperplastic type (candidal leukoplakia) (Fig. 3.3) Figure 3.3 Chronic hyperplastic candidiasis with no wipeable white surface.
Site—usually anterior buccal mucosa; tongue.
Morphology—plaque.
Color—white.
Signs and symptoms—cannot be scraped off and so cannot be clinically distinguished from leukoplakia. Candidal leukoplakia often can have a red component intermingled (i.e., speckled leukoplakia).
Treatment—antifungal agents (cream, ointment, liquid, tablets). If the lesion fails to resolve (essentially confirming the diagnosis), then a biopsy is mandatory.
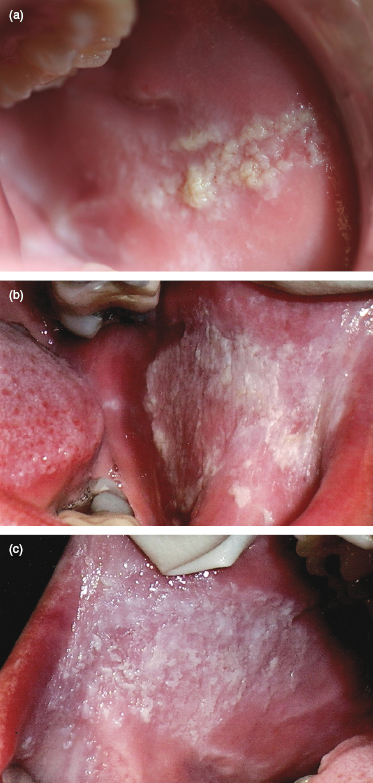
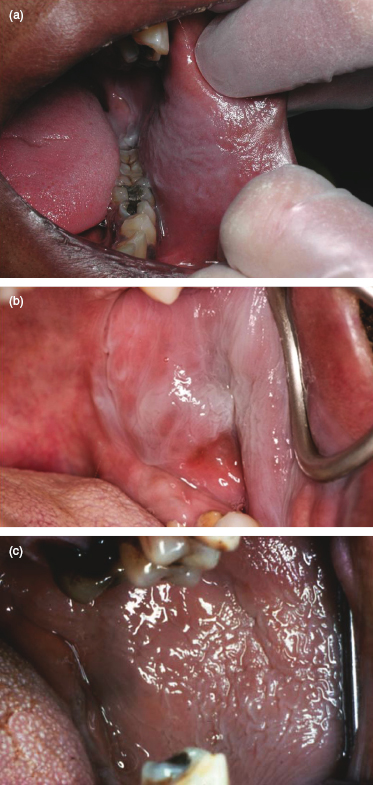
Morsicatio (nibbling habit) (Fig. 3.4a,b,c) Figure 3.4 (a) Mild case of chronic cheek nibbling (i.e., morsicatio buccarum) above and below the occlusal plane. (b and c) Extensive chronic cheek nibbling with numerous white wipeable tissue tags and nonwipeable white base.
Site—most often buccal mucosa (morsicatio buccarum) centered along occlusal plane; also labial mucosa (morsicatio labiorum), lateral tongue (morsicatio linguarum).
Morphology—roughened, ragged, thickened surface plaque; may also see ulceration and erosion intermixed.
Color—white.
Signs and symptoms—a conscious or subconscious chronic nibbling habit or, rarely, suction; asymptomatic. The superficial portion (i.e., tissue tags) can be scraped or peeled off but the remainder cannot. Lesions are usually bilateral, with or without other site involvement.
Treatment—none required.
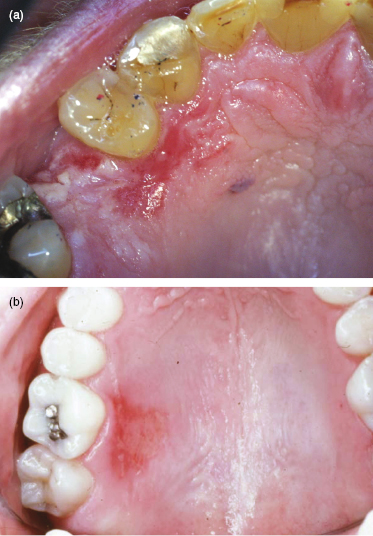
Thermal burn (Fig. 3.5a,b) Figure 3.5 (a) Thermal burn of the lateral anterior hard palate secondary to hot food. (b) Thermal burn of the lateral posterior hard palate.
Site—palate or posterior buccal mucosa.
Morphology—red macule (erythema) with ulcer, often with remnant of epithelium at the periphery.
Color—white.
Signs and symptoms—usually results from history of accidental ingestion of hot foods or beverages. Superficial white change can be scraped off or is wipeable due to surface coagulative necrosis.
Treatment—resolves without treatment.
Chemical burn (aspirin burn) (Fig. 3.6a,b) Figure 3.6 (a) Chemical burn (i.e., aspirin burn) secondary to direct application of analgesic to the oral mucosa due to odontogenic pain. (b) Extensive chemical burn (i.e., aspirin burn) secondary to direct application of analgesic to the oral mucosa due to pericoronitis.
Site—all oral mucosal sites.
Morphology
Short exposure time—superficial wrinkled plaque.
Longer exposure time—surface epithelium becomes separated from underlying tissue, easily desquamates into erosion.
Signs and symptoms—history of accidental oral mucosal contact with caustic agents such as aspirin, hydrogen peroxide, silver nitrate, phenol, and endodontic materials. Overuse of mouthwashes with high alcohol content can also cause a superficial white slough of the mucosa. If the exposure time was long, then the surface is removable, leaving red bleeding connective tissue with subsequent formation of a yellow-gray fibrinopurulent membrane (can be scraped off).
Treatment—prevention of exposure. Superficial damage resolves without scarring in 10–24 days, during which a protective emollient paste or a hydroxypropyl cellulose film can be applied; for larger, deeper damage surgical debridement and antibiotic coverage are used.
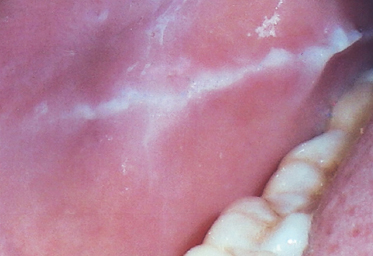
Linea alba (Fig. 3.7) Figure 3.7 Linea alba due to mild frictional keratosis of the buccal mucosa’s occlusal plane.
Site—buccal mucosa, occlusal plane; unilateral or bilateral and symmetrical distribution.
Morphology—thin linear plaque.
Color—white.
Signs and symptoms—asymptomatic; caused by frictional irritation, pressure, or sucking trauma from the facial surfaces of the teeth; cannot be wiped off.
Treatment—none. It is considered a common variation of normal.
Leukoedema (Fig. 3.8a,b,c) Figure 3.8 (a–c) Leukoedema (spongiosis) of the buccal mucosa.
Site—buccal mucosa; bilateral and symmetrical distribution.
Morphology—diffuse, plaquelike; often has delicate overlapping curtainlike mucosal folds.
Color—translucent white-gray.
Signs and symptoms—asymptomatic. Leukoedema is significantly more common in Blacks and other dark-skinned persons. The abnormal color tends to dissipate or disappear when the buccal mucosa is stretched.
Treatment—none.
Leukoplakia (Fig. 3.9) Figure 3.9 Snuff dipper’s keratotic leukoplakia of the posterior buccal mucosa at the site where the smokeless tobacco product is held.
Site—lip vermilion, buccal mucosa, gingiva; also tongue, floor of mouth, soft palate, and hard palate.
Morphology—patch or plaque; thin or homogeneous (thick) or nonhomogeneous (nodular, granular, verruciform), proliferative; distinct margins.
Color—gray to gray-white to white; may be intermixed with red (i.e., speckled leukoplakia).
Signs and symptoms—clinical term, defined as white patch or plaque that cannot be characterized clinically or pathologically as any other disease (i.e., diagnosis of exclusion); asymptomatic; may show keratosis, dysplasia, or invasive carcinoma; caused by tobacco, alcohol, ultraviolet radiation, microorganisms (e.g., Treponema pallidum, Candida albicans, and HPV types 16 and 181–8), and trauma; there is also an idiopathic form; occurs more often in older individuals. A variant, known as “hairy” leukoplakia, is seen most commonly on the lateral tongue, in an uncontrolled HIV-positive patient; it results from an Epstein–Barr infection, and its name is based on roughened elongations of the surface epithelium.
Treatment—biopsy is mandatory to obtain a histopathologic diagnosis. If dysplasia is present, then complete removal should be verified with long-term follow-up since a 4% transformation rate to squamous cell carcinoma has been reported.
Actinic cheilitis (cheilosis) (Fig. 3.10a,b,c,d) Figure 3.10 (a) Sun-damaged lower lip vermilion with actinic cheilitis. (b) Actinic cheilitis of the lower lip vermilion. (c) Actinic cheilitis of the lower lip vermilion exhibiting mottled colors and indistinct border with the skin. (d) Actinic keratosis with epithelial dysplasia and early invasive squamous cell carcinoma.
Site—lower lip vermilion border.
Morphology—rough plaque and scale, which thickens with time; ulcer late.
Color—blotchy, pale gray-white.
Signs and symptoms—usually seen in older men (10:1 male-to-female ratio) with a history of chronic or excessive ultraviolet exposure from sun, tanning salons, and so on, especially those with light complexion and easily sunburned; considered a potentially malignant (i.e., precancerous) lesion. There is blurring of the margin between the vermilion zone and the cutaneous lip. The scale can, at times, be peeled off with some difficulty and then recurs within days. Actinic cheilitis is similar to actinic keratosis of the skin.
Treatment—Indurated, thickened scale or ulcer should be biopsied to rule out dysplasia or carcinoma (6–10% transformation rate reported). If malignant transformation occurs, then treat with lip shave (i.e., vermilionectomy) surgically or with laser ablation, electrodesiccation, topical chemicals (e.g., topical 5-fluorouracil, imiquimod), photodynamic therapy, or chemoexfoliation with trichloroacetic acid. Long-term follow-up is recommended. Preventive measures include lip balm and sunscreen.
Lichen planus
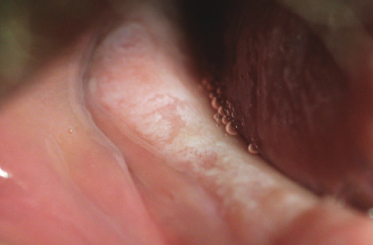
Reticular type (Fig. 3.11) Figure 3.11 Classic reticular oral lichen planus of the anterior and posterior buccal mucosa.
Site—chronic cutaneous disease that can also affect the oral mucosa. Posterior buccal mucosa is most often affected; also, gingiva, palate, labial mucosa, and lateral/ventral tongue; distribution is usually bilateral and symmetrical.
Morphology—papules; solitary and multiple lesions that coalesce into an interlacing network of white lines known as Wickham’s striae.
Color—white.
Signs and symptoms—cannot be scraped off; usually asymptomatic. Reticular lichen planus occurs more often in middle-aged adults, women 3:2 over men. The condition waxes and wanes over weeks to months.
Treatment—biopsy often needed for diagnosis confirmation. If asymptomatic, no treatment is needed; if mild burning sensation, usually due to secondary candidiasis, then antifungal therapy is needed. Some clinicians advocate annual reevaluations even if asymptomatic.
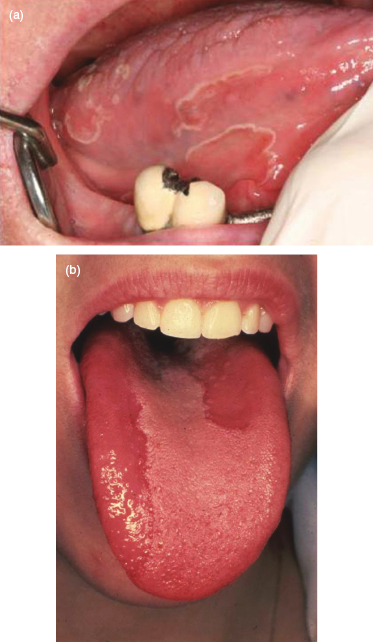
Hypertrophic type (Fig. 3.12) Figure 3.12 Hyperplastic (leukoplakic) lichen planus of the dorsal tongue.
Site—most often on dorsal tongue.
Morphology—plaque.
Color—white.
Signs and symptoms—cannot be scraped off; asymptomatic. Hypertrophic lichen planus occurs more often in middle-aged adults, women 3:2 over men. The condition waxes and wanes over weeks to months.
Treatment—if asymptomatic, no treatment is needed; if mild burning sensation, usually due to secondary candidiasis, then antifungal therapy is needed. Some clinicians advocate annual reevaluations even if asymptomatic.
Alveolar ridge keratosis (Fig. 3.13) Figure 3.13 Benign alveolar ridge keratosis, which microscopically will demonstrate hyperkeratosis without dysplasia.
Site—edentulous maxillary or mandibular alveolar mucosal areas especially without removable prosthesis present.
Morphology—plaque with variable surface roughness.
Color—white.
Signs and symptoms—painless; due to friction of mastication.
Treatment—usually observation. However, the lesion can be biopsied to rule out dysplasia.
Red-and-White Lesions
Geographic tongue (benign migratory glossitis, erythema migrans) (Fig. 3.14a,b) Figure 3.14 (a) Geographic tongue (also called benign migratory glossitis, erythema migrans) with flat red areas encircled by raised white rim. (b) Geographic tongue with red flat areas but lacking classic white raised border.
Site—anterior two-thirds of dorsal tongue, also lateral and ventral. It is much rarer on other sites such as buccal mucosa, labial mucosa, and soft palate (but with the same morphology and colors) and is referred to as ectopic geographic tongue.
Morphology—multiple, well-demarcated macule(s) from atrophy of filiform papillae surrounded completely or partially by a slightly elevated, scalloped border.
Color—red macule and yellow-white border.
Signs and symptoms—occurs 2:1 female-to-male ratio; asymptomatic or variable burning sensation or tongue sensitivity to hot or spicy foods. Lesions usually quickly develop in one area, heal in days to weeks, then develop in a different area; geographic tongue is often associated with fissured tongue.
Treatment—usually none. If there is a burning sensation and lifestyle is disrupted, then prescribe topical steroids (gel or rinse formulations).
Candidiasis, chronic multifocal type (Fig. 3.15) Figure 3.15 Chronic multifocal type of candidiasis.
Site—posterior dorsal tongue. Other sites include the labial commissures and the posterior hard palate, the latter due to swallowing in which the posterior tongue “kisses” the hard palate.
Morphology—macules and plaques.
Color—red macules and white plaques.
Signs and symptoms—associated with immunosuppression or idiopathic; removable white plaque; asymptomatic or burning sensation.
Treatment—antifungal agents.
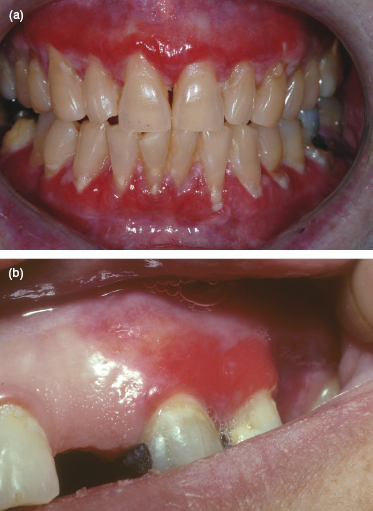
Lichen planus, atrophic and erosive types (Fig. 3.16a,b) Figure 3.16 (a) Bilateral and symmetrical distribution of erosive lichen planus of the facial attached gingiva. (b) Focal lesions of erosive lichen planus of the left maxillary facial attached and marginal gingiva.
Site—posterior buccal mucosa, usually bilateral; gingiva; also lateroventral tongue, floor of mouth, soft palate.
Morphology—plaque, macule; shallow ulceration, erosion; periphery of white lines.
Color—red macules, erosions; white papules, plaques.
Signs and symptoms—pain. In severe cases an epithelial separation from the underlying connective tissue may occur, resulting in ulceration.
Treatment—usually a biopsy is necessary to rule out lupus erythematosus as well as the presence of dysplasia. Medications usually include topical corticosteroids and, in recalcitrant cases, systemic corticosteroids.
Nicotine stomatitis (Fig. 3.17) Figure 3.17 Bilateral nicotine stomatitis of the hard palate.
Site—hard palate; bilateral and symmetrical distribution.
Morphology—palate has slightly elevated papules, often with cobblestone or pebbly surface. Advanced lesions may have a “dried mud” or fissured appearance; plaques on gingiva and buccal mucosa.
Color—diffuse gray to white with punctate red centers on hard palate (inflamed minor salivary gland ductal orifices).
Signs and symptoms—usually seen in pipe smokers (heat-induced) but in some ethnic groups “reverse smoking” (lit end of cigarette within the oral cavity) can be the cause. It also can be seen with a chronic habit of hot beverage consumption.
Treatment—completely reversible (1–2 weeks) with tobacco habit cessation. Nicotine stomatitis is not a premalignant lesion.
Erythroleukoplakia (speckled leukoplakia) (Fig. 3.18) Figure 3.18 Extensive erythroplakia of the soft palate.
Site—any oral mucosal surface.
Morphology—patch or plaque intermixed with soft, velvety texture; distinct margins.
Color—gray-white to white intermixed with red.
Signs and symptoms—clinical term, defined as a white-and-red patch or plaque that cannot be characterized clinically or pathologically as any other disease (i.e., diagnosis of exclusion); asymptomatic; caused by tobacco, alcohol, microorganisms (e.g., Treponema pallidum, Candida albicans, HPV types 16 and 181–8), and trauma. There is also an idiopathic form. Erythroleukoplakia occurs more often in older individuals.
Treatment—biopsy, particularly including the red component, is mandatory to obtain a histopathologic diagnosis. If dysplasia is present, then complete removal should be verified with long-term follow-up since the red component has a significant transformation rate to severe dysplasia or worse (i.e., 90% or greater).
Allergic reactions (Fig. 3.19) Figure 3.19 Lichenoid contact allergic reaction (i.e., stomatitis venenata) of the posterior buccal mucosa secondary to cinnamon aldehyde flavoring agent.
Site—posterior buccal mucosa and posterior lateral border of tongue are most commonly involved, usually with bilateral and symmetrical distribution; any other mucosal site, including labial vermilion or dorsal tongue. In fixed drug eruption reaction the site of involvement is the same each exposure time.
Morphology—macule, vesicles (temporary), erosions, superficial ulcerations (red); local contact may also have white patches and plaques. Artificial cinnamon flavoring and dental restorative materials as well as drugs (i.e., lichenoid mucositis) are common triggers.
Color—red and white.
Signs and symptoms—systemic drugs, contact with substances and dental restorative materials; usually burning sensation, paresthesia, or variable pain; edema may be present (systemic drugs). Allergic reactions may have the clinical appearance of pemphigus, pemphigoid, lichen planus, lupus erythematosus, chronic ulcerative stomatitis, or aphthouslike ulcers.9
Treatment—eliminate allergen; supplement with topical or systemic corticosteroid; epinephrine or antihistamine therapy for edema; depending on acute or chronic onset nature.
Red Lesions
Candidiasis
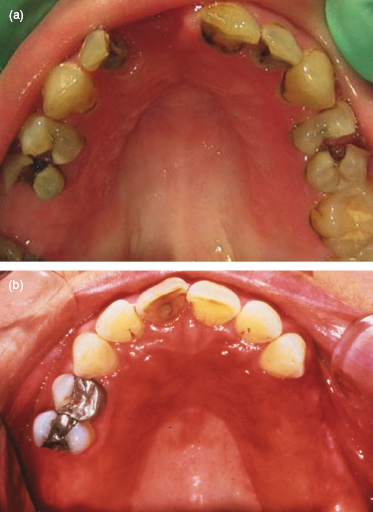
Chronic atrophic type (denture stomatitis, denture sore mouth) (Fig. 3.20a,b) Figure 3.20 (a) Chronic atrophic candidiasis of the maxilla beneath an acrylic removable denture. (b) Chronic atrophic candidiasis of the hard palate beneath a removable partial denture.
Site—denture-bearing mucosa of maxillary removable dental prosthesis, especially the palate.
Morphology—well demarcated macule.
Color—red
Signs and symptoms—rarely symptomatic. The patient usually wears the prosthesis continually, only removing it to clean. It is somewhat controversial if this is truly a fungal infection or is just an association since biopsied tissue does not demonstrate the hallmark of an infection: host tissue invasion by the organism (i.e., the denture but not the mucosa has a positive culture result).
Treatment—treat both mucosa and prosthesis base with antifungal agents.
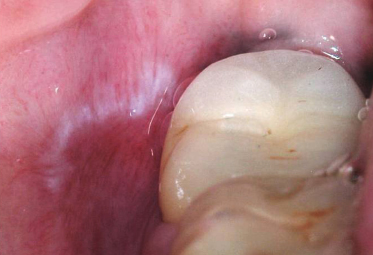
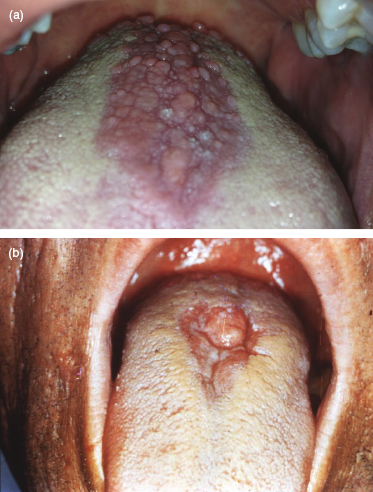
Chronic erythematous type, median rhomboid glossitis (central papillary atrophy) (Fig. 3.21a,b) Figure 3.21 (a) Median rhomboid glossitis (chronic erythematous candidiasis), flat and raised, at the midline junction of the anterior two-thirds and posterior one-third of the dorsal tongue. (b) Median rhomboid glossitis (chronic erythematous candidiasis) of the posterior dorsal tongue.
Site—midline dorsal surface of tongue just anterior to the circumvallate papillae.
Morphology—smooth macule or lobulated papule.
Color—red.
Signs and symptoms—often asymptomatic; results from loss of the filiform papillae. Distribution is usually symmetrical.
Treatment—usually resolves completely with antifungal agent but often recurs.
Angular cheilitis (perleche) (Fig. 3.22) Figure 3.22 Angular cheilitis (perleche) of the left commissure due to chronic erythematous candidiasis.
Site—commissures (angles) of the lip.
Morphology—fissures and scales within folds of tissue.
Color—red.
Signs and symptoms—unilateral or bilateral; caused by persistent wetness (e.g., loss of vertical dimension), immunosuppression, nutritional deficiencies (e.g., vitamins), and infections of, commonly, Candida albicans or, rarely, Staphylococcus aureus. There is also an idiopathic form. Severity can wax and wane.
Treatment—usually resolves completely with an occlusive dressing, to block moisture, and an antifungal agent. Sometimes it requires antibiotic as well as antifungal agent to eliminate Staphylococcus aureus presence.
Geographic tongue (Fig. 3.23a,b,c) Figure 3.23 (a) Flat, irregular, discontinuous areas of geographic tongue. (b) Flat red areas of geographic tongue in a child. (c) Ectopic geographic tongue (erythema migrans) of the middle lower labial mucosa.
Lesions have the same characteristics as described previously (“Red-and-White Lesions,” number 1) except that the white, slightly raised elevated periphery is lacking.
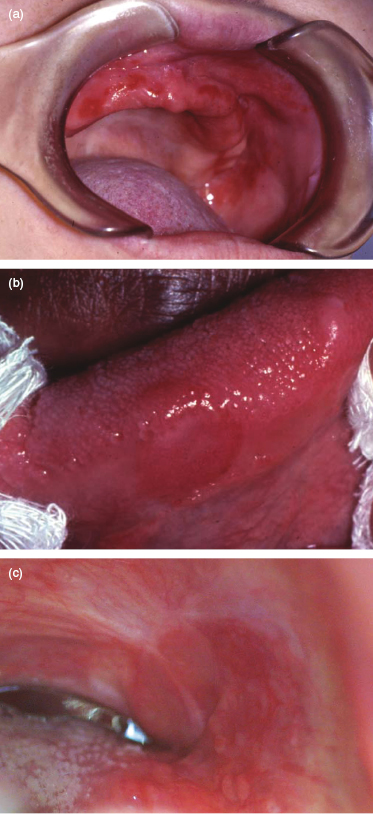
Erythroplakia (Fig. 3.24a,b,c,d) Figure 3.24 (a) Erythroplakia (also called speckled leukoplakia) with microscopic carcinoma-in-situ in a patient immunosuppressed following a bone marrow transplant. (b) Erythroplakia of the middle one-third lateral border of the tongue. (c) Erythroplakia of the left tonsillar fossa area. (d) Subtle erythroplakia at the mucogingival junction of the left maxillary central incisor area.
Site—tongue, floor of mouth, soft palate.
Morphology—macule, patch, or plaque with soft, velvety texture.
Color—red.
Signs and symptoms—clinical term, defined as a red patch or plaque that cannot be characterized clinically or pathologically as any other disease (i.e., diagnosis of exclusion); usually asymptomatic; atrophy with usually severe dysplasia, in situ carcinoma, or invasive carcinoma; caused by tobacco, alcohol; idiopathic form also; occurs more often in middle-aged to older adults. Multiple lesions may be present.1–3
Treatment—biopsy is mandatory to obtain a histopathologic diagnosis and 90% or more have at least severe dysplasia. There should be long-term follow-up for treated patients since there is the likelihood of recurrence or a new primary lesion at the same site or other oral mucosal site.
Hemangioma (vascular malformations) (Fig. 3.25) Figure 3.25 Unilateral hemangioma of a patient with Sturge–Weber syndrome.
Site—head and neck skin; tongue, buccal mucosa, labial mucosa.
Morphology—macule, vesicle, or bulla.
Color—red, red-blue, blue.
Signs and symptoms—present at birth (i.e., congenital) or during infancy although may not be clinically apparent until later. Cherry hemangiomas of the lips typically arise in middle age. Hemangiomas are compressible and blanchable.
Treatment—spontaneous involution sometimes; systemic corticosteroid, laser, or sclerotherapy and surgical excision.
Extravasated blood
Site—any oral mucosal site.
Morphology—macule or elevated.
Color—red, red-blue, blue.
Signs and symptoms—usually due to trauma. Lesions do not blanch with pressure.
Treatment—spontaneously resolve unless due to systemic disease (i.e., control the associated disease). Large hematomas may require several weeks to resolve.
Macular type—submucosal hemorrhage resulting in entrapment of a thin layer (i.e., not a mass) of extravasated blood within the tissues. Lesions do not blanch with pressure and are named based on size of the greatest diameter:
Petechia—0.1–2 cm; round pinpoint area of hemorrhage (Fig. 3.26) Figure 3.26 Multiple pinpoint petechiae of the lower lip vermilion and labial mucosa.
Purpura—0.3–2.0 cm; nonelevated area of hemorrhage larger than a petechia (Fig. 3.27) Figure 3.27 Purpura of the lower lip secondary to trauma.
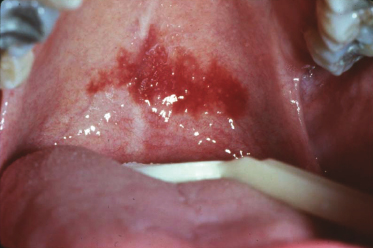
Ecchymosis—greater than 2.0 cm; nonelevated area of hemorrhage larger than a purpura (Fig. 3.28) Figure 3.28 Petechiae and ecchymosis at the junction of the soft and hard palate.
Elevated type—submucosal hemorrhage resulting in entrapment of a thick layer (i.e., elevated mass) of extravasated blood within tissue. The lesion does not blanch with pressure; the name is not size dependent:
Hematoma (Fig. 3.29) Figure 3.29 Elevated hematoma (bulla) of the right anterior lateral tongue.
Telangiectasia (Fig. 3.30) Figure 3.30 Telangiectasias of the lips in a patient diagnosed with hereditary hemorrhagic telangiectasia.
Site—lip vermilion, tongue, buccal mucosa; any other oral mucosal site.
Morphology—papules (1–2 mm).
Color—red.
Signs and symptoms—caused by dilatation of small capillaries close to the surface. Lesions blanch when compressed (positive diascopy).
Treatment—no treatment except if hereditary hemorrhagic telangiectasia disease (nosebleeds, gastrointestinal bleeding), then moderate cases require cryosurgery, electrocautery, or laser ablation; and severe cases, surgery.