Orthodontics
Learning Objectives
1 Pronounce, define, and spell the Key Terms.
2 Identify the classifications of malocclusion.
3 Describe the types of records utilized for the orthodontist to make a diagnosis and treatment plan.
4 Describe the categories of orthodontic treatment.
5 Identify and describe the function of orthodontic instruments.
6 Describe the purpose of attachments, auxiliaries, and arch wires in corrective orthodontics.
Key Terms
Arch Wires
Auxiliaries
Bands
Cephalometric
Fixed Appliances
Headgear
Malocclusion
Open Bite
Removable Appliances
Retainer
Separator
Tipping
Orthodontics is the specialty of dentistry that includes the diagnosis, prevention, interception, and treatment of all forms of malocclusion of the teeth and surrounding structures. (Malocclusion is an abnormal or malpositioned relationship of the maxillary teeth to the mandibular teeth when occluded.)
Types of treatment include straightening teeth that are rotated, tilted, or improperly aligned, or crowded or unevenly spaced; correcting bite problems; and aligning the upper and lower jaws.
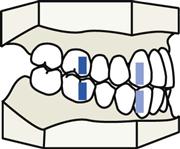
Angle’s Classifications of Malocclusion
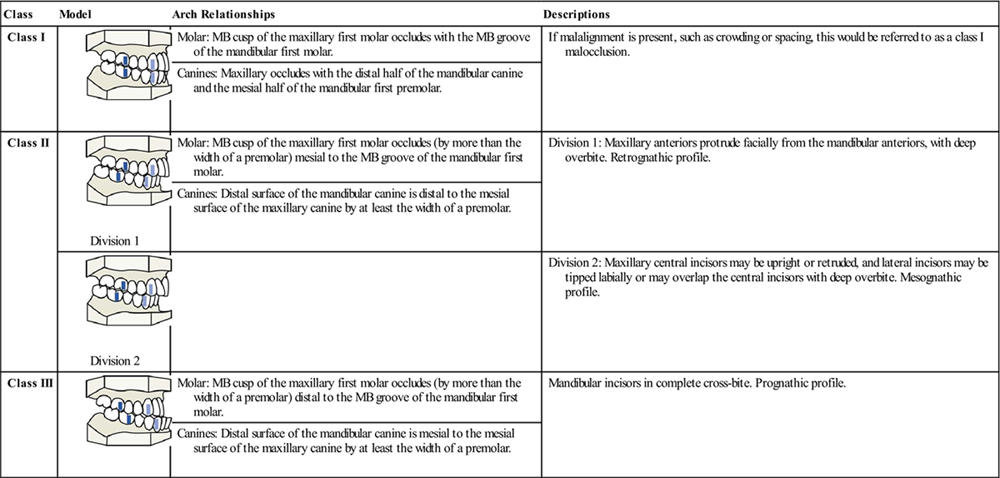
The system developed by Dr. Edward H. Angle is used to describe and classify occlusion and malocclusion. In this system, the key to understanding the relationship of a person’s “bite” is identifying the relationship of the permanent first molars when the patient is in centric occlusion. See Table 28-1 for further clarification.
TABLE 28-1
Angle’s Classification of Malocclusion*
< ?comst?>
| Class | Model | Arch Relationships | Descriptions |
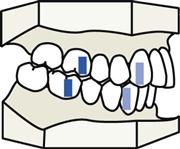
| Class I |
 |
Molar: MB cusp of the maxillary first molar occludes with the MB groove of the mandibular first molar. | If malalignment is present, such as crowding or spacing, this would be referred to as a class I malocclusion. |
| Canines: Maxillary occludes with the distal half of the mandibular canine and the mesial half of the mandibular first premolar. | |||
| Class II |
 Division 1 |
Molar: MB cusp of the maxillary first molar occludes (by more than the width of a premolar) mesial to the MB groove of the mandibular first molar. | Division 1: Maxillary anteriors protrude facially from the mandibular anteriors, with deep overbite. Retrognathic profile. |
| Canines: Distal surface of the mandibular canine is distal to the mesial surface of the maxillary canine by at least the width of a premolar. | |||
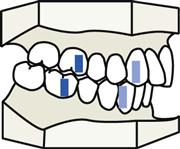 Division 2 |
Division 2: Maxillary central incisors may be upright or retruded, and lateral incisors may be tipped labially or may overlap the central incisors with deep overbite. Mesognathic profile. | ||
| Class III |
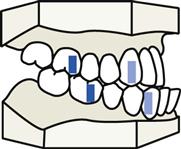 |
Molar: MB cusp of the maxillary first molar occludes (by more than the width of a premolar) distal to the MB groove of the mandibular first molar. | Mandibular incisors in complete cross-bite. Prognathic profile. |
| Canines: Distal surface of the mandibular canine is mesial to the mesial surface of the maxillary canine by at least the width of a premolar. |
< ?comen?>< ?comst1?>
< ?comst1?>
< ?comen1?>
< ?comst1?>< ?comen1?>*< ?comst1?>< ?comen1?>Note: This system deals with the classification of permanent dentition.
All illustrations from Bath-Balogh M, Fehrenbach MF: Illustrated dental embryology, histology, and anatomy, ed 3, St Louis, 2011, Saunders.
Indications for Orthodontic Treatment
Orthodontic treatment may be necessary as a result of any combination of the following conditions:
Records Visit and Treatment Planning
The first orthodontic appointment is scheduled to obtain records required by the orthodontist to make a diagnosis and create a treatment plan. The patient’s diagnosis is based on information from three major sources:
Interview Information
The orthodontist requires information that is gathered by interviewing the patient and/or parent/guardian.
Medical and Dental History
A thorough medical and dental history is necessary to provide a comprehensive understanding of the physical condition and to evaluate specific orthodontically related concerns.
Physical Growth Evaluation
Because orthodontic treatment in children is closely related to growth stages, it is necessary to evaluate the child’s physical growth status. Questions include how rapidly the child has grown recently and what signs of sexual maturing are evident.
Social and Behavioral Evaluation
Motivation for seeking treatment is very important. What does the patient and the parent/guardian expect as a result of treatment? How cooperative or uncooperative is the patient likely to be?
A major motivation for orthodontic treatment of children is the parents’ desire for treatment; however, it is essential that the child be willing and cooperative.
Adults seek orthodontic treatment for themselves for other reasons. These reasons include the need to improve personal appearance or function of the teeth. Whichever the reason, it is important to explore why the patient seeks treatment at this time.
Clinical Examination
The purpose of the orthodontic clinical examination is to document and evaluate the facial aspects, the occlusal relationship, and the functional characteristics of the jaws. At the records visit, the orthodontist decides which diagnostic records are required for the patient.
Evaluation of Facial Form
Facial form analysis is the visual examination of the face. It provides information that cannot be gathered from dental radiographs and diagnostic casts (Figure 28-1).

Frontal evaluation (from the front)—the orthodontist examines the face for:
Profile evaluation (from the side)—the orthodontist examines the face in profile to:
Evaluation of Oral Health
A thorough hard and soft tissue examination and an oral hygiene assessment must be completed before orthodontic treatment begins. If problems are detected, the patient is referred for preventive and restorative treatment before orthodontic treatment is started.
Diagnostic Records
Diagnostic records include photographs, radiographs, and diagnostic casts which provide data related to tooth angulation, dental crowding, and the presence of unerupted teeth. When possible, it is best to have these available at the time of the clinical examination.
Photographs
Photography is useful as an aid in patient identification, treatment planning, case presentation, case documentation, and patient education and instruction.
Extraoral Photographs.
Two standard extraoral photographs are taken: (1) the frontal view, with lips in a relaxed position; and (2) a profile view of the patient’s right side, with lips in a relaxed position (Figure 28-2).

Intraoral Photographs.
Three standard intraoral photographs are also required: (1) the full direct view, which includes all teeth in occlusion; (2) the maxillary occlusal view, which includes the palate and all maxillary occlusal surfaces; and (3) the right buccal view, which includes the distal of the canine to the distal of the last molar (Figure 28-3).



Radiographs
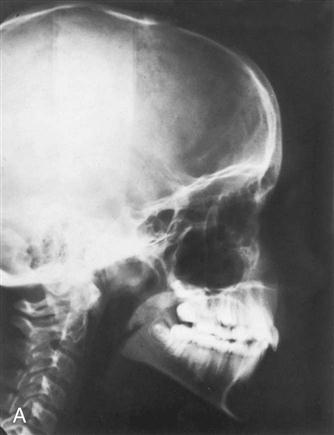
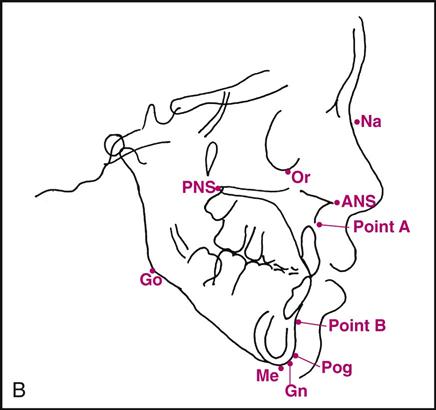
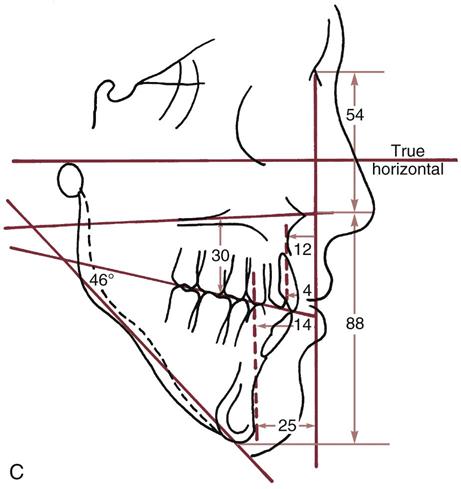
Cephalometric Radiograph.
A cephalometric radiograph is an extraoral radiograph that is exposed from a side view, showing how the major functional skeletal structures of the face are related to each other (Figure 28-4). This makes it possible for the orthodontist to measure and evaluate dentofacial proportions and to clarify the anatomic basis for a malocclusion.
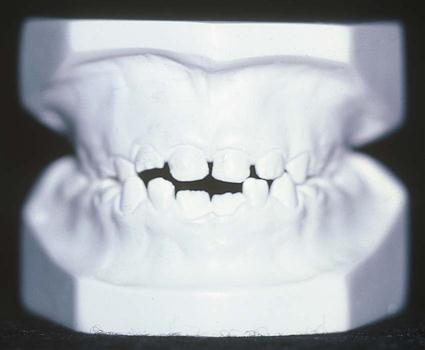
Diagnostic Casts
Evaluation of the occlusion requires impressions for diagnostic casts and a record of the patient’s occlusion so the casts can be articulated. Alginate impressions and diagnostic casts are discussed in Chapter 22.
For orthodontic purposes, the diagnostic casts are trimmed so that the bases have a symmetric shape that is oriented to the midline of the palate. This makes it much easier to detect asymmetry within the dental arches. The casts should be polished so that they will be more acceptable for presentation to the patient (Figure 28-5).
The Case Presentation
The orthodontist studies the information gathered and develops a treatment plan and a cost estimate for the patient in preparation for the case presentation.
Approximately 1 hour is reserved for the case presentation visit, and the patient—and parent or responsible adult if the patient is a child—should be present. This presentation includes the approximate length of treatment, the fees involved, and a clear statement of the responsibility of the patient in helping to ensure successful completion.
Orthodontic Treatment
Orthodontic treatment can be divided into four broad categories: preventive, limited, interceptive, and comprehensive.
Preventive Orthodontic Treatment
Preventive orthodontic procedures are designed to prevent or minimize the degree of severity of future orthodontic problems.
This treatment, which is commonly provided by the pediatric or general dentist, includes:
Limited Orthodontic Treatment
This category includes orthodontic treatment with a limited objective that would not involve the entire dentition. An example would be the correction of an open bite with a fixed or removable appliance.
Limited treatment may be directed at the only existing problem or at only one aspect of a larger problem for which a decision is made to defer or forego more comprehensive therapy.
Interceptive Orthodontic Treatment
Interceptive treatment is an extension of preventive and/or limited orthodontics but may include localized tooth movement in an otherwise normal dentition.
This treatment usually occurs in the transitional dentition and may include such procedures as redirection of a tooth that has erupted out of position, correction of an isolated cross-bite, or recovery of lost space where overall space is not adequate.
Another interceptive step is the serial extraction of primary or permanent teeth to correct critical overcrowding in the arch. This is performed only when more conservative methods of treatment will not be effective. When extractions are required, the orthodontist refers the patient to a general dentist or to an oral and maxillofacial surgeon.
Comprehensive Orthodontic Treatment
Comprehensive orthodontic treatment involves coordinated diagnosis and treatment leading to improvement of the patient’s craniofacial dysfunction and/or dentofacial deformity, including anatomic, functional, and esthetic relationships. This type of treatment uses fixed orthodontic appliances.
Fixed appliances, commonly known as braces, are attached to the teeth and assist in tooth movement (Figure 28-6). These appliances are discussed later in this chapter.

Removable appliances, which can be placed and removed by the patient, are not used to produce major tooth movement. Instead they are used primarily as retainers (after comprehensive treatment) or in tipping teeth. (Tipping is the movement of a tooth into a more upright position.)
Instruments for Orthodontics
Orthodontics requires the use of highly specialized instruments. Listed are the most common types. See Table 28-2 for names and descriptions of use.
TABLE 28-2
Orthodontic Instruments and Their Uses
< ?comst?>
| Instrument | Description of Use |
Orthodontic scaler
 |
Aids in bracket placement, removal of elastomeric rings, and removal of excess cement or bonding material. |
Ligature director
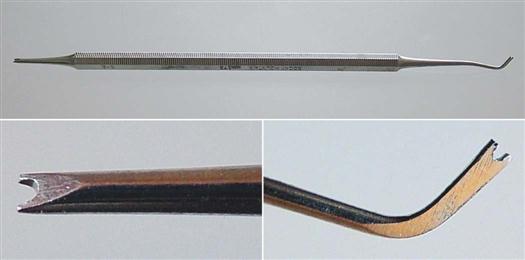 |
Guides the elastic or wire ligature tie around the bracket. Additionally, the operator can guide the cut tie under the arch wire. |
| Band plugger/pusher |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


