chapter 24 Venipuncture Technique
PREPARATION OF EQUIPMENT







Figure 24-6 If the drip chamber is overfilled, the bag is inverted, and the chamber is squeezed to remove solution.
Additional equipment required for venipuncture includes the following:
PREPARATION FOR VENIPUNCTURE
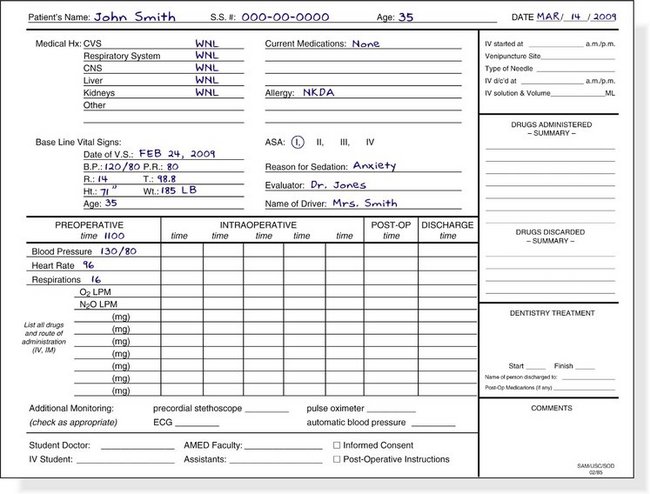
Preoperative vital signs are recorded on the patient’s sedation record sheet (Figure 24-7). Included should be the blood pressure, heart rate and rhythm, respiratory rate, and O2 saturation. The patient’s baseline vital signs have been recorded at a prior visit to the dental office.
The patient’s arms (without the tourniquet in place) are scanned for obvious veins. Often veins will be made readily visible if the arm is permitted to hang down below the level of the patient’s heart for a few minutes because this augments venous distention (Figure 24-8). One of the goals of the preoperative visit was to determine whether the patient has suitable veins for the IV procedure.

If the Trieger test for evaluation of recovery is to be used (see Chapter 5), the baseline Trieger test is now completed by the patient. Any other monitoring devices, such as the pulse oximeter, capnograph, pretracheal stethoscope, or electrocardioscope, are now placed on the patient.
A tourniquet is placed on the limb (arm or leg) selected for venipuncture. On the arm, the tourniquet is placed superior to the antecubital fossa. The commonly used soft rubber tubing (e.g., Penrose drain) is applied in a slipknot (Figure 24-9). The tourniquet should be sufficiently tight to prevent venous drainage from the arm without obstructing arterial flow into the arm. A radial pulse should still be palpable with the tourniquet in place.


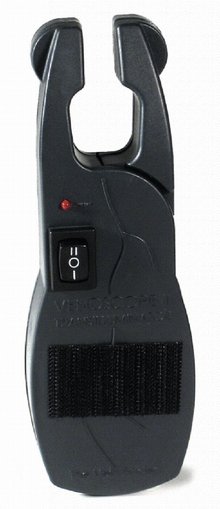
Figure 24-10 Vein locating device (www.med1online.com).
(Courtesy Venoscope, L.L.C., Lafayette, LA.)
When N2O-O2 is used as an aid during venipuncture, the patient should be sedated as described in Chapter 15 (titrated) and returned to a nonsedated state before the administration of any IV drugs.
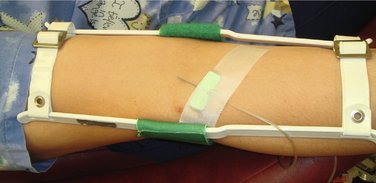
Once the vein chosen for cannulation has been adequately distended, the site must be prepared. Physical restraints are seldom required in adults because most patients rarely object strenuously to venipuncture (although they may not “like it”). When a vein in the antecubital fossa or wrist is selected, an elbow or wrist immobilizer should be placed before the start of the venipuncture if a rigid metal needle is to be used (Figure 24-11). An immobilizer is unnecessary if a flexible catheter is to be inserted.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


