23
The Use of Humor in Pediatric Dentistry
- The use of humor in pediatric dentistry is highly recommended.
- It may be used to facilitate communication with patients and parents.
- Humor may alleviate patient anxiety and assist the dentist in coping with stress associated with the practice of dentistry.
- Development of humor in the child is described.
- Practical suggestions for application of humor in daily pediatric dental practice are presented.
For many years, studies have suggested that dentistry generates more stress than any other profession, primarily because of the nature and working conditions of the dental practice (Bodner, 2008). It is recognized that dentistry is a stressful profession in general, and in particular, the specialty of pediatric dentistry can be all the more stressful. Crying children, overprotective and sometimes outright hostile parents, coupled with a child’s small mouth and teeth all contribute to a stressful environment. The introduction of humor into the daily practice of pediatric dentistry may have a compounding double effect by alleviating the stressed patient and at the same time allowing the dentist to cope on a daily basis with the stress faced everyday while treating young dental patients. The use of humor for the management of both children patients and their involved parents will be discussed in this chapter.
While some might consider humor’s playful role trivial, findings point to its critical role in building and maintaining relationships, emotional health, and cognitive function (Martin, 2007). Pediatric dentists anecdotally have long recognized the presence of humor in their practice; yet planned humor assessment and interventions are relatively recent considerations in medicine/dental care. Humor has positive effects on both a person’s physiology and psyche. Laughter signifies positive things to people; it may add to feelings of togetherness, closeness, and friendliness. The use of humor is an indication of mental well-being. It minimizes the effect of negative factors and protects from difficulties. An understanding of humor development and associated activities will assist pediatric dentists to (a) anticipate the various types of humor unique to each stage of childhood, (b) develop individualized humor interventions, and (c) evaluate the outcomes of these humor interventions (Dowling, 2002).
Definitions
Prior to further discussion, a synopsis of common theories and definitions of humor are in order. A full discourse on humor theory is beyond the scope of this review, but certain basic definitions are essential. From a psychological perspective, humor involves cognitive, emotional, behavioral, psycho-physiological, and social aspects (Mora-Ripoll, 2010). In general, the term humor can refer to a stimulus, which is intended to produce a humorous response (such as a humorous video), a mental process (perception of amusing incongruities), or a response (laughter, exhilaration). Laughter is the most common expression of humorous experience. Humor and laughter are also typically associated with a pleasant emotional state. For the purpose of this discussion, humor is defined as a stimulus that helps people laugh and feel happy. Laughter is a psychophysiological response to humor that involves both characteristic physiological reactions and positive psychological shifts. Sense of humor is a psychological trait that varies considerably and allows persons to respond to different types of humorous stimuli. It is necessary to differentiate between these variables (Mora-Ripoll, 2010).
Theories of Humor
Three main theories explain the functions of humor: the relief theory, which focuses on physiological release of tension; the incongruity theory, which focuses on contradictions between expectations and experiences; and the superiority theory, which focuses on sense of supremacy over others (Wilkins & Eisenbraun, 2009). Each theory accounts for the role of humor in specific situations: relief humor for relaxing tensions during social interactions, incongruity humor for presenting new perspectives, and superiority humor for criticizing opposition or unifying a group. The purpose that humor serves in any given situation may be open to interpretation, but the physiological effects are not. Cognition is needed to understand humor, but it is not needed for the physiological effects of laughter to occur. In other words, individuals will experience similar bodily reactions regardless of whether they laugh due to tension release or through appreciation of incongruities. A brief description of the three main theories about the functions of humor follows.
Relief Theory
According to the relief theory, people experience humor and engage in laughter because they sense that stress is reduced in doing so (Kuiper, Martin, & Olinger, 1993). Alternately, people may laugh at something humorous, which then results in a feeling of mirth and sense of relief. Relief may involve a cognitive release from anxiety or a physical release of tension (Wilkins & Eisenbraun, 2009). The physiological benefits of laughter most closely align with this theoretical perspective as many negative health conditions are exacerbated by stress, and laughter has been shown to reduce the symptoms of such conditions. In individuals with bronchial asthma, for example, negative emotional states, can induce airway constriction, while positive emotional states can relieve airway constriction. Thus humor and laughter, and the resulting emotion, mirth, can unite the body and mind (Dossey & Keegan, 2008).
Incongruity Theory
The incongruity theory purports that people laugh at things that surprise them or at things that violate an accepted pattern—with a difference close enough to the norm to be nonthreatening, but different enough from the norm to be remarkable it will be further discussed in the next section. Briefly, the incongruity theory emphasizes cognition; individuals must have rationally come to understand typical patterns of reality before they can notice differences (Wilkins & Eisenbraun, 2009). A humorous situation must involve the perceiver’s simultaneously having in mind one view of the situation that seems normal and another view of the situation in which there is a violation of the natural order (Veatch, 1998). This theory has support in neuroimaging research, which shows that the parts of the brain involved in resolving incongruities are activated while processing cartoons (Samson et al., 2009).
Superiority Theory
The superiority theory proposes that laughing at faulty behavior can reinforce unity among group members (Duncan, 1985). It is believed that superiority humor serves two important societal functions: it maintains social order as laughter, rather than aggression, is invoked toward those who refuse to comply with rules, and through laughing together at others, it reinforces group unity (Long & Graesser, 1988), (Martineau, 1972). While the latter may seem like a malicious form of humor, it is one that we encounter surprisingly often. There are many television shows based on this very form of humor—Candid Camera and the multitude of spin-offs, for example, base their comedy on people caught in foolish and embarrassing situations (Wilkins & Eisenbraun, 2009).
Development of Humor in the Child
Pediatric dentists who are interested in helping young patients use humor effectively need to understand the developmental aspects of humor. A child’s capacity to appreciate humor depends on their cognitive and sensory abilities, prior experiences, and stages of development. Changes in basic patterns of humor at different ages depend on underlying changes in intellectual development. A simple approach to the development of humor is based on the above-mentioned concept of incongruity. The term refers to absurdity, nonsense, and irony. Incongruity is considered as an essential element in the production and appreciation of humor. McGhee (1979) defined humor as the mental experience of discovering or appreciating ludicrous or absurdly incongruous ideas, events, or situations. Sense of humor develops parallel to emotional and intellectual development. Researchers have investigated the age during which the ability to recognize incongruities arises and have related it to other cognitive abilities that children might be develop, such as symbolic play (Loizou, 2006).
Using a cognitive approach to humor, Paul E. McGhee developed a theory which traces the development and appreciation of humor in children through defined stages and continues to form the framework for research in this area. Each stage is based on the children’s cognitive abilities that enable the child to recognize and produce cognitive incongruities. Taking a cue from Piaget’s cognitive stages, McGhee first proposed a comprehensive stage-model of children’s humor in 1979, linking the stages of humor development to Piagetian stages of intellectual development (Loizou, 2006). This model maps the type of humor the child is likely fascinated with to underlying changes in the child’s ability to perceive and make sense of its world (Cunningham, 2005). The stages, as defined by McGhee were (1) incongruous actions toward objects; (2) incongruous labeling of objects and events; (3) conceptual incongruity; and (4) humor in multiple meanings (Table 23.1). Chronological ages may vary among individuals from one stage to another, but the sequence is thought to be identical for all (Dowling, 2002). McGhee refined the earlier definitions and published a new system of stages introducing five stages, including a prehumor stage as described in 2002 (McGhee, 2002). A summary and description of these stages is presented and are of practical benefit to the pediatric dentist using humor in the dental setting.
Table 23.1 Comparison of Piaget’s (1962) Cognitive Stages of Child Development with McGhee’s (1979, 2002) Proposed Stages of Humor Development
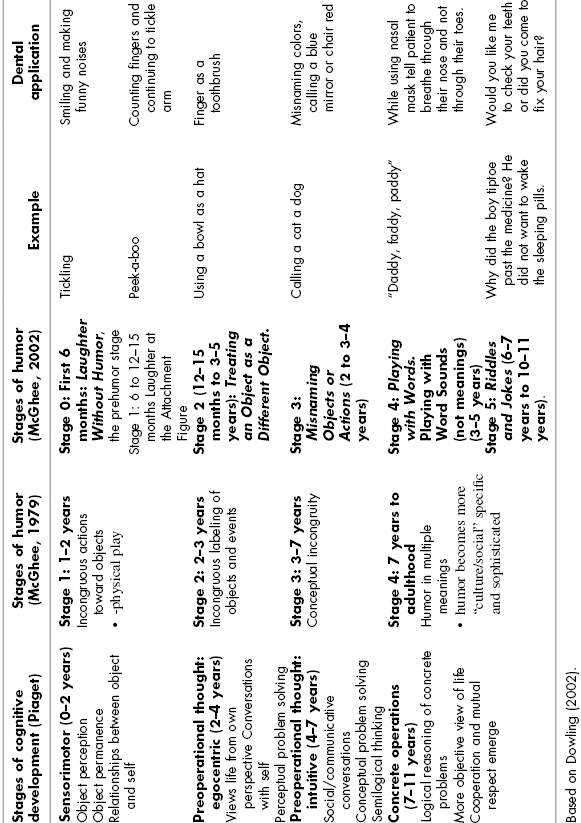
Piaget’s first stage of child development (0–2 years), sensorimotor development, is concerned with the perception and permanence of objects as well as the relationships between objects and self (Dowling, 2002). The infant explores the world through direct sensory and motor contact. This Piaget stage may be divided into two in relation to the child’s humor development: the prehumor stage and first stage of humor development.
Stage 0 (first 6 months): Laughter without Humor, the prehumor stage. Although, during its first month of life, an infant may exhibit smiling and even laughter, it is a result of spontaneous activity of the central nervous system; however, toward the end of the first month of life, the first wakeful smile appears and tends to occur after feeding. Research on infants suggests that anything that is physiologically arousing to them, in a familiar or nonthreatening situation, can trigger laughter (McGhee, 2002). Pleasurable sensations, such as blowing, can elicit laughs over and over again. All forms of tactile stimulation yield laughter: bouncing the infant on one’s knee, quickly lowering the baby, or tickling are reliable causes of laughter. An unexpected noise such as clapping may result in either laughing or crying. By age 4 months, a broader smile connected to a broader range of events including moving objects or lights appears. The infant begins to respond to visual human items and not only to tactile stimuli (such as kissing stomach, lip popping).
Stage 1 (6 to 12–15 months): Laughter at the Attachment Figure. In this stage, the infant demonstrates an increasing awareness of its interpersonal surroundings and participates in social humor with a parent or other attachment figure through visual and aural games. The baby responds to visual and social items such as mother sucking on a bottle, father waddling like a penguin, any unusual behavior of the attachment person and disappearing objects. Objects do not fit the schema into which they are being assimilated (Loizou, 2006). They are temporarily used in a way that differs from an ordinary one, such as in a game of “peek-a-boo.” The child looks for the puppet on one side of the crib and then erupts in laughter when it unexpectedly shows up on the other side. In addition, the infant still enjoys physical social stimuli, reacting with laughter to vigorous physical play like throwing the baby in the air or tickling.
Stage 2 (12–15 months to 3–5 years): Treating an Object as a Different Object. At stage 2, children begin producing “jokes” nonverbally by performing incongruous actions, such as putting a bowl on their head as a hat or pretending to talk into their shoe, any incongruous action with an object. Another form of typical humor is using the correct object, but applying it to the wrong object, for example, the child may ask: “Brush ear?” In these cases, the same behavior may be just as funny if it is the mother, father, or another sibling who initiates it (McGhee, 2002). The child’s frame of mind determines whether it’s humor or not. This stage is significant since it presents the earliest self-created humor. This stage is the parallel of incongruous actions toward objects from the initial McGhee system of humor development and corresponds to Piaget’s Sensorimotor stage (Object perception, Object permanence, and relationships between object and self).
Stage 3: Misnaming Objects or Actions (2 to 3–4 years). Once the child’s vocabulary hits a critical point, the young child can extend incongruity humor to misnaming objects or actions: calling a cat a dog, a shoe a sock. After age two, parents are asked by their child to name people and things. Toddlers are very excited by the realization that everything has a name and begin playing with the names of things. Many parents first see this new form of humor in the “Show me your nose” game. Even if the parent has always played the game straight, the day always arrives when the child is prompted to “Show me your nose,” and exhibits a mischievous grin and points to his or her ear. The child may or may not laugh, but there’s no doubt that this is pretty funny to them. McGhee notes that children at this stage often enjoy calling things by their opposite name—cold as hot, boy as girl. While humor based on using objects in “wrong” ways continues throughout the peak of pretend behavior during the preschool years, budding language skills generate new opportunities for humor. The previous equivalent stage is incongruous labeling of objects and events corresponding to Piaget’s Preoperational Thought: Egocentric (views life from own perspective, conversations with self, and perceptual problem solving).
Stage 4: Playing with Words. Playing with Word Sounds (not meanings) (3–5 years). As the child’s verbal competence grows, he or she is less dependent on objects as the source of humor. The preschooler may experiment with rhyming words, made-up silly words, and other humorous play that does not directly link to concrete objects within their reach. Many children are especially fond of the verbal expression of humor found in stories and poems like The Cat in the Hat (Seuss, 1957). Humor includes playing with word sounds—not meanings, altering funny words, creating nonsense words. Several new forms of humor emerge by the end of the third year. Simply calling things by the wrong name continues to be funny after age two, but a new way of playing with words appears around age three. Children become much attuned to the way words sound/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


