Reconstruction of Congenital Auricular Malformations
Anatomy and Embryology
Topographic landmarks of a normal ear are shown in Figure 23-1. Development of the auricle is first observed in the 5-week-old embryo. The auricle begins as six mesenchymal proliferations at the dorsal ends of the first and second pharyngeal arches surrounding the first pharyngeal cleft. Initially, the external ear is located in the lower neck of the embryo. As the mandible develops, the ear ascends to the side of the head at the level of the eyes. The commonly accepted embryologic theory (Fig. 23-2) is that the six hillocks correlate directly with the tragus, helix, cymba, scapha, antihelix, and antitragus.1
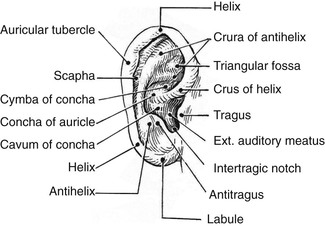
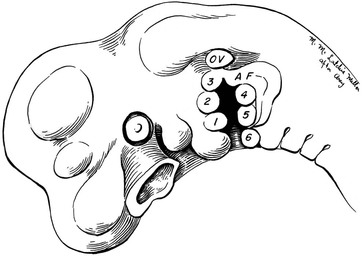
FIGURE 23-2 Auricle in 5-week human embryo develops from six hillocks. OV, otic vesicle; AF, auricular fold.
A normal auricle is shown in Figure 23-3. The vertical axis of the normal auricle is tilted posteriorly approximately 20°. The vertical height of the normal ear is approximately equal to the distance between the lateral bony orbital rim and the root of the helix at the level of the eyebrow (about 6-cm). The width of the ear is approximately 55% of its height. Typically, the helical rim protrudes 1- to 2-cm from the skull, and the angle of protrusion should be between 25° and 30°. The superior aspect of the ear is usually level with the eyebrow.2

Preoperative Considerations
A number of congenital auricular deformities exist that may require surgical intervention. To achieve the most natural appearing ear possible through surgery, the surgeon must assess the deformed ear for the presence of several important auricular landmarks. Recognizing and grading the deformity will allow the surgeon to craft the proper surgical options. Involving family members of the patient with an ear deformity is important. Eavey3 observed that children with microtia and significant auricular malformations require comprehensive attention directed to early family counseling and evaluation of the patient for expected and unexpected hearing loss, impaired language development, and associated medical conditions. Both auricular and otologic reconstructive procedures may be necessary and must be coordinated. In 1999, Wang4 identified that the early use of an auricular prosthesis is psychologically beneficial to children who have an ear defect resulting from congenital malformation. Wang also described techniques to establish the proper location and orientation of auricular implants used to secure auricular prostheses by using information from computed tomography (CT) scans. The techniques were applied to children and adults to ensure accurate implant placement, leading to improved positioning and orientation of auricular prostheses.
Congenital Malformations
External ear deformities exist in 1% of births. Correcting major congenital malformations of the auricle tests the plastic surgeon’s surgical skills. Microtia has been the subject of numerous publications as clinicians have attempted to establish a method of classification of the severity of a given deformity. Tanzer5,6 in 1959 published the first scientific article on auricular reconstruction with autogenous rib cartilage. In 1966, Cronin7 popularized the use of silicone as an implant material to reconstruct auricles. Brent,8 who first reported his work in 1974, is considered the world’s foremost authority on auricular reconstruction.
Classification
In 1988, Aguilar and Jahrsdoerfer9 amended the 1926 grading system used to classify the severity of microtia described by Marx. In 1996, Aguilar10 reaffirmed this concise classification of congenital ear malformations: grade I is a normal ear; grade II has some of the auricular framework present, but there are obvious deformities; and grade III is the standard “peanut ear” deformity (Fig. 23-4), which encompasses anotia (Marx’s grade IV).


In 1977, Tanzer11 proposed a clinical classification of auricular deformities. This has been used by others and consists of the following:
Complete hypoplasia (microtia)
Hypoplasia of the middle third of the auricle
In 1974, Rogers12 published a similar classification that divided deformities into four groups: macrotia, lop ear, cup ear, and prominent ear. Weerda13 combined all of the classifications proposed by Marx and Tanzer and modified by Rogers.14 This classification is included for completeness, and demonstrates the awkwardness of classification schemes that are too comprehensive or detailed. Weerda’s system included surgical guidance for each classification:
First-degree dysplasia. Average definition: most structures of a normal auricle are recognizable (minor deformities). Surgical definition: reconstruction normally does not require the use of additional skin or cartilage.
Protruding ears; synonyms: prominent ears, bat ears
Cryptotia; synonyms: pocket ear, group IV B (Tanzer)
Small deformities: absence of the tragus, satyr ear, darwinian tubercle, additional folds (Stahl ear)
Colobomas; synonyms: clefts, transverse coloboma
Lobule deformities; synonyms: pixed lobule, macrolobule, absence of lobule, lobule colobomas (bifid lobule)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


