CHAPTER 20 Preliminary Prosthodontics: Fabricating a Template
FULLY EDENTULOUS JAW
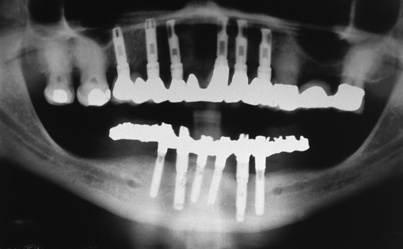
At this point, the treatment plan is finalized. Choices of a device and other elements are made on the basis of available bone and its quality; the patient’s capabilities, aspirations, and finances; and the dental surgeon’s skills and prejudices. The resulting prosthesis may be an overdenture totally supported by the tissue and retained by an O-ring or ball attachments. It may use two implants, three or more implants (with a fixed cemented or fixed-detachable mesostructure bar, which may be partly or fully implant supported), or five or more implants (buttressing an anatomic fixed bridge or a bar-borne hybrid fixed prosthesis) (Fig. 20-1). Whatever arrangement is chosen, the completed support mechanism (abutments, attachments, bars) must fit within the confines of the newly completed denture. If this cannot be done, the envisioned final appliance will be too large, which will create possibly insoluble esthetic and functional problems.
The denture, therefore, plays a significant role in the processes of planning, management, and fabrication of the complex restorative device. If the patient already wears a denture that satisfies the required tooth and flange positions, it can be replicated for use in creating the appliance. However, if the existing prosthesis is unacceptable, a new one that presents correct functional and esthetic characteristics must be made.
Replication of the Trial Denture
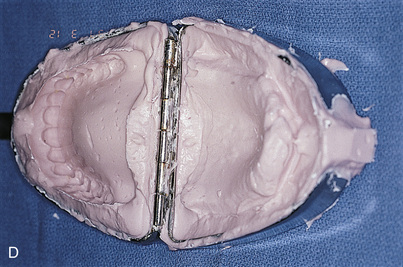
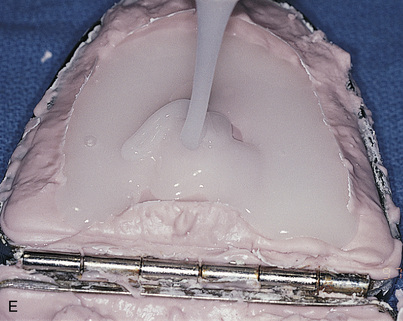
The trial denture is replicated for use as a surgical template in the following manner.
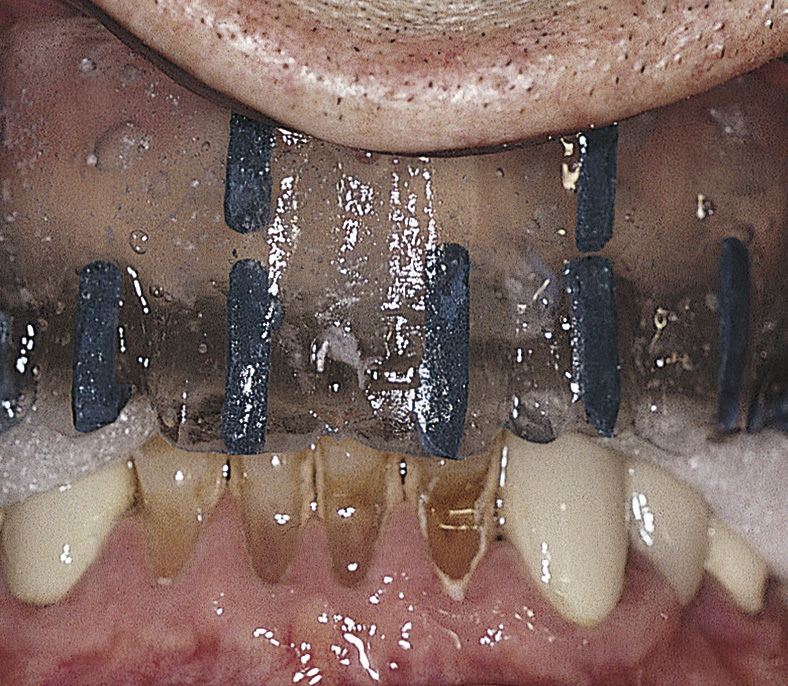



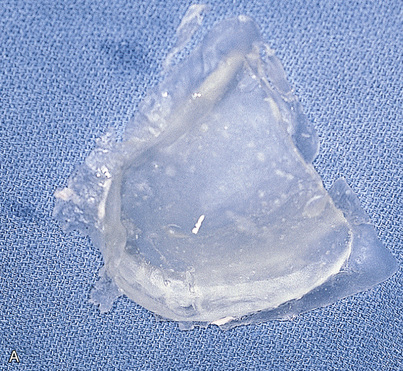




The clear acrylic denture fulfills its first critical function in presurgical CT scanning. Chapter 4 describes in detail the techniques for embedding a radiopaque medium into premeasured grooves; this process is essential for verifying the locations and dimensions of host sites intraoperatively (see Fig. 20-2). Adding a 3-mm occlusal run to the appliance stabilizes the jaw and provides comfort in the resting position.
After the appliance had been used for CT scanning, it can be used as a surgical template. However, an additional alteration is required. The occlusal incisal edge and lingual acrylic of all potential implant host sites must be cut away (Fig. 20-7). This allows surgical access to the bone while the template occupies its anatomic position. The radiopaque markers allow the surgeon to transfer image findings and dimensions directly to the bony host sites (see Chapter 4).

Surgical templates are necessary to position implants accurately and predictably. Two different designs of surgical templates are recommended for partially edentulous areas. The first style replicates the provisional denture restoration and is made on the corrected replicated cast. The second style uses an Omnivac template but relies on adjacent teeth and soft tissues for support and positioning. If more than two implants are planned, the surgical template that replicates the provisional prosthesis, rather than the Omnivac template, should be used (Fig. 20-8).

FIGURE 20-8. An example of a template for a partially edentulous patient. In this case, the template was fabricated from an acceptable acrylic partial denture in a manner described for complete templates. As an alternative to this procedure, a template can be fabricated based on a suitable wax-up (see Chapter 4).
The first steps are the physical and radiologic examinations of the patient (see chapters 3 and 4). The implantologist then decides which planning method to use (model based or computer based). The fabrication company (e.g., SciCat [Sirona], Procera [Nobel Biocare], Navigator system [Biomet-3i]) provides the necessary components to create a customized surgical template. Based on the design of the surgical template, they also supply the implants and the surgical and laboratory instruments required to facilitate the operation.
Before surgery, the surgeon can have a temporary or final prosthesis fabricated that can be attached in the same session as the implant installation.
MODEL-BASED PLANNING
Definitions
ARMAMENTARIUM
The conventional approach to implant surgery follows these steps:
The computer-guided approach shortens the interval between surgery and the final prosthesis:
The results are significantly reduced chair time and increased profitability
Computer-Based Treatment Planning and Surgery
If the patient has only a few teeth in the opposing jaw and does not wear a partial prosthesis, the surgeon must make sure to fill the area where the teeth are missing with occlusion index material to make contact with the alveolar ridge. This ensures a horizontal, well-balanced bite registration. The radiographic guide is used to simulate the teeth, soft tissue surface, and edentulous space during the CT scan.
NOTE
MODEL-BASED PLANNING AND PROCEDURE WITHOUT A THREE-DIMENSIONAL SCAN

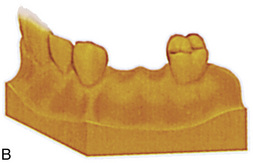

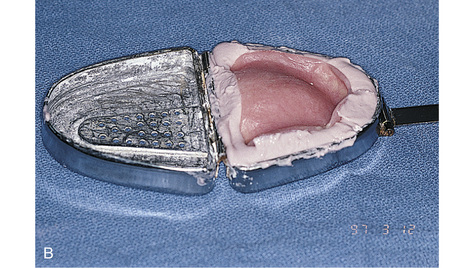
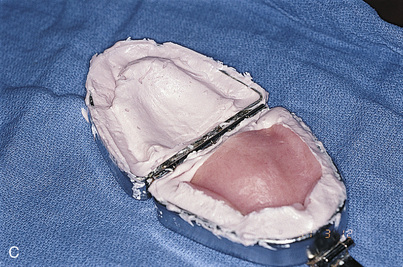
FIGURE 20-9. A-C, Model-based planning without a three-dimensional scan.
(Courtesy Nobel Biocare, Yorba Linda, Calif.)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


