Restorative Considerations in Occlusal Therapy
“RESTORING THE TEETH IS FUNDAMENTAL TO THE PRACTICE OF DENTISTRY.”
—JPO
IN THE GENERAL PRACTICE OF DENTISTRY, the greatest number of procedures are in some form restorative. The rationale for providing this treatment is the replacement or rebuilding of missing tooth structure. Unfortunately the influence that these procedures have on the occlusal condition of the teeth is often underemphasized. Most restorative procedures cannot be performed without influencing to some degree the existing occlusal condition. The potential effect of restorative procedures on the occlusion is obvious when a complete reconstruction of the dentition is being considered. However, one should be aware that even an occlusal amalgam can have a significant effect on the occlusion when the restoration is under- or overcarved.
On occasion, a series of small and seemingly insignificant changes will occur slowly over an extended period, resulting in a gradual loss of occlusal stability. These often go unnoticed by the patient until significant occlusal interferences have resulted. By contrast, abrupt changes in the occlusion are usually quickly noticed by the patient and therefore are often resolved before difficult consequences arise.
It is important to consider that all restorative procedures are, in some degree, a form of occlusal therapy. This statement is not always true, however, since some restorations do not replace occluding surfaces (e.g., a buccal pit restoration on a mandibular first molar or an anterior crown for a patient with an anterior open bite). Nevertheless, the vast majority of restorations do involve occluding surfaces. Since restorative procedures can affect the occlusal condition, when it is determined that occlusal therapy is indicated to resolve a temporomandibular disorder (TMD), restorative procedures can often provide the necessary occlusal changes to meet the treatment goals. Since restorative procedures utilize both addition and subtraction of tooth surfaces, a greater degree of occlusal change can be accomplished with these than with selective grinding only.
Restorative procedures and occlusal therapy should generally be considered inseparable. When restorative procedures are indicated primarily to eliminate dental caries and rebuild teeth, care must be taken to redevelop a sound functional occlusion. When they are indicated primarily as occlusal therapy, the same care must be taken to rebuild the teeth to sound esthetics and a form compatible with the adjacent tissues.
In this chapter, restorative procedures are divided into two types: operative and fixed prosthodontic. Operative procedures are those in which the final restorations are fabricated intraorally (e.g., an amalgam, a composite resin). Fixed prosthodontic procedures are those that involve extraoral fabrication with final adjustment and cementation in the mouth (e.g., inlays, onlays, full crowns, fixed partial dentures). Although in this chapter little emphasis is placed on the removable partial denture, the same occlusal considerations are appropriate with regard to it.
Operative Considerations in Occlusal Therapy
It is unfortunate that when operative techniques are discussed in the literature little emphasis is usually placed on occlusal considerations. The success or failure of the procedure, however, relies not only on the margins and contours of the restoration but equally on the occlusal relationship.
Treatment Goals
To stabilize a tooth and provide optimal functional conditions, one must accomplish certain treatment goals. These can be divided into (1) tooth contacts and (2) mandibular position.
Treatment goals for tooth contacts
Posterior contacts
After an operative procedure, the new restoration must provide stability of both the opposing and the adjacent teeth so that drifting or eruption will not occur. When the mandible closes, the new restoration must provide for even, simultaneous, and harmonious occlusion with the existing posterior tooth contacts. It should direct forces through the long axes of the teeth. In many cases, prior to the restoration this stability and axial loading have been provided by reciprocating inclines as a cusp fit into an opposing fossa. Carving an amalgam back into a reciprocating incline contact relationship is often a difficult task. If it is attempted and full reciprocation is not achieved (missing an incline), instability can result. Therefore it is frequently best to develop the necessary stability and axial loading by carving the restoration to type of contact relationship where a cusp tip opposes a flat surface. This will fulfill the treatment goals.
Anterior Contacts
The majority of operative procedures completed on the anterior teeth are composite resin restorations and should restore the teeth to normal form and function. One occlusal requirement of the anterior teeth (as indicated in Chapter 5) is to provide guidance for the mandible during eccentric movement. Therefore the anterior teeth should contact with less force than the posterior teeth in the closing position. During an eccentric movement, available anterior teeth should guide the mandible and disocclude the posterior teeth. In the head-upright position (alert feeding position), the anterior teeth should not contact as heavily as the posterior teeth.
Treatment goals for the mandibular position
When operative procedures are performed, the mandibular position at which the restorations are developed depends largely on the presence of any functional disturbance of the masticatory system. When operative procedures are performed on a patient with no functional disturbances, the restorations are generally developed in the maximal intercuspal position (ICP). If a patient has a functional disturbance of the masticatory system, it is generally best to resolve it before the operative procedure begins. If, in resolving the disorder, it is determined that the occlusal condition is a major etiologic factor, then a selective grinding procedure (when found to be feasible) should be completed before any operative procedures. Thus the restorations can be developed into the sound occlusal relationship achieved by the selective grinding procedure.
Accomplishing the Treatment Goals
The likelihood of accomplishing the treatment goals for both anterior and posterior teeth is greatly enhanced by closely examining the occlusal conditions prior to the operative procedure. This is done by visualizing diagnostic casts or by having the patient close on articulating paper and marking the occlusal contacts. Knowing the location of the existing contacts can greatly assist in reestablishing these contacts on the restoration.
Posterior contacts
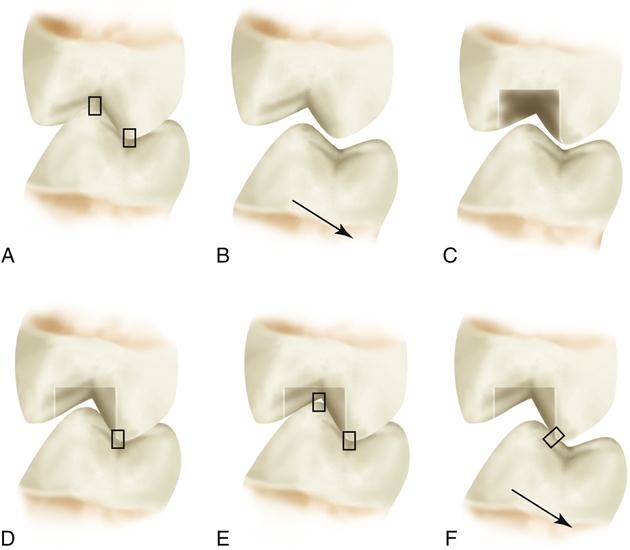
Reestablishing stable posterior tooth contacts on a new amalgam restoration can be a trying task. One quickly learns that leaving a new amalgam restoration too high often results in fracture of the restoration and the need for replacement. Therefore a great tendency exists to overcarve the amalgam slightly and thus protect the setting amalgam from fracture. Although the immediate results may be satisfying, since the patient cannot detect any alteration in the occlusion, the condition that has been developed is usually unstable, allowing for drifting or eruption of the teeth until new occlusal contacts can be established. This drifting can result in undesirable tooth relationships and/or eccentric contacts (Figure 20-1).
Therefore amalgam restorations should be carved into and not out of occlusion. Initially the patient is asked to close gently on articulating paper and the excess amalgam is carved away. By observing the occlusal contact prior to the operative procedure, one can gain valuable insight regarding the location and extent of carving that must be completed. The area of setting amalgam that opposes a centric cusp tip is carved to a flat surface. Depending on its location, the flat area will be either a marginal ridge or a central fossa. It is helpful to examine for contacts on natural tooth structure. When these occur, the carving of the restoration is nearly complete. After it has been determined that the restoration is contacting evenly and simultaneously (on cusp tips and flat surfaces) with the opposing teeth, eccentric contacts are evaluated. A different-colored marking paper is helpful in identifying the eccentric contacts from the closing contacts (as in the selective grinding procedure, discussed in Chapter 19). In most instances amalgam restorations do not serve as guidance surfaces for mandibular movement and eccentric contact is therefore completely eliminated. The same principles are observed in placing posterior composite restorations.
Anterior contacts
The initial guide used to develop anterior composite restorations is tooth morphology. When the composite is shaped and finished to the tooth’s original contour, the occlusal condition is evaluated. Heavy contacts in the desired mandibular closure position are reduced. Frequently these can be detected by placing the fingers on the labial surfaces of the teeth while the patient closes and taps on the posterior teeth (Figure 20-2). Heavy contacts tend to displace the teeth labially or cause heavy vibration (known as fremitus). These contacts are marked and adjusted until the fingers cannot detect any unusual displacement of the restored teeth.

When the contacts in mandibular closure have been adjusted, eccentric mandibular movements are observed. If a restoration is involved with an eccentric pathway, it should provide a smooth and unrestricted movement. Any irregularity of its surface must be smoothed to enhance this movement. A restoration that has been overcarved or overpolished, leaving a distinct catch or defect on its margin, is replaced. It is evaluated not only in straight protrusive and laterotrusive movements but also through various lateroprotrusive excursions.
When the restoration is adequately adjusted to the eccentric movements, the patient is brought upright in the dental chair and the alert feeding position is evaluated. Heavy contacts on the anterior teeth are reduced until the posterior teeth become more prominent.
Fixed Prosthodontic Considerations in Occlusal Therapy
Fixed prosthodontics afford many advantages in occlusal therapy over operative procedures. Although operative procedures involve replacing tooth surfaces, the occlusal condition is usually developed by careful removal of restorative material. In this sense, they are subject to the same limitations as selective grinding. Fixed prosthodontics, however, utilizes the benefit of adding and subtracting tooth surfaces until the precise desired restoration is achieved. Since this is accomplished most often extraorally, errors stemming from poor intraoral working conditions (i.e., visibility, access, saliva) are avoided. With the appropriate use of articulators (Chapter 18), restorations can be fabricated precisely to meet treatment goals. Once these steps are completed, final adjustments are made in the mouth.
Treatment Goals
As with operative procedures, the treatment goals for fixed prosthodontics can be divided into tooth contacts and mandibular position.
Treatment goals for tooth contacts
Posterior contacts
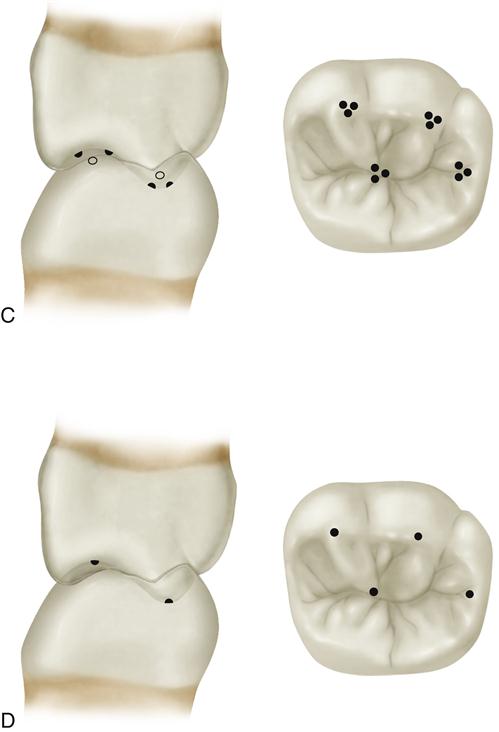
The posterior teeth should contact in a manner that provides stability while directing forces through the long axes of the teeth. Since precise tooth form can be developed, this axial loading may be accomplished by utilizing reciprocating incline contacts around the centric cusps (known as tripodization) or by developing a contact from cusp tip to opposing flat surface (Figure 20-3). Both methods will achieve the treatment goals.
Anterior contacts
The anterior teeth should come into light contact during closure while providing prominent contact during eccentric movements. Since fixed prosthodontic procedures allow for greater control of the entire tooth form, the precise guidance pattern can be more carefully controlled. As with other procedures, the alert feeding position must not create heavy anterior tooth contacts.
Treatment goals for the mandibular position
The mandibular position to which the fixed prosthodontic restorations are fabricated is determined by two factors: (1) the presence of any functional disturbance in the masticatory system and (2) the extent of the procedures indicated.
Functional disturbances
A thorough examination of the patient must be performed prior to any fixed prosthetic procedures. If any functional disturbance is noted, it is treated and resolved before the procedures begin. If it is determined by reversible occlusal therapy and the other considerations discussed in Chapter 15 that the existing occlusal condition is a contributing etiologic factor, a selective grinding procedure is completed so that a stable occlusal condition is developed in the desired mandibular position (CR). Once this occlusal relationship has been established, the fixed restorations are developed to stabilize the occlusal condition and mandibular position.
Extent of treatment
In patients with no signs of functional disturbance of the masticatory system, the extent of fixed prosthodontics indicated determines the mandibular position to be used in restoring the occlusion. Patients with no functional disturbance basically demonstrate that their occlusal condition falls within their physiologic tolerance.
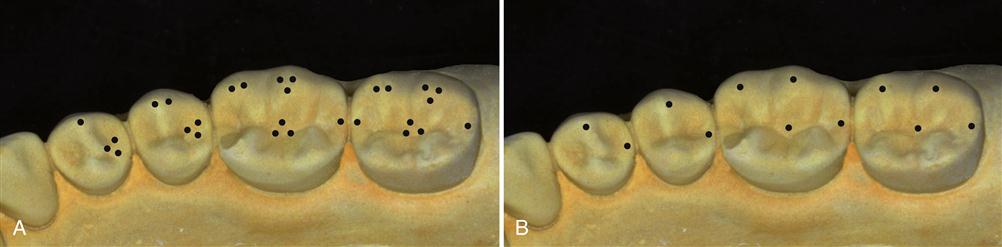
When minor fixed restorative procedures are indicated (e.g., a single crown), it is appropriate for the restoration to be developed in harmony with the existing occlusal condition (Figure 20-4). Therefore/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


