Chapter 2
Normal Anatomy
Aim
To demonstrate the normal radiological anatomy visible on intraoral radiographs.
Introduction
It is impossible to recognise abnormality without first being familiar with normality and its variants. For dentists, the radiological anatomy of greatest importance is that of the teeth and surrounding bony structures. Of course, a single anatomical diagram or radiograph cannot serve as a blueprint for all patients: bony anatomy has normal variations. However, recognition of normal “patterns” of tooth and bone is the surest way of spotting pathosis when it is present.
Teeth and the Periodontium
Experience shows that normal features of teeth are occasionally interpreted as abnormal. Therefore we make no apology for starting with “the basics”.
The Tooth
The tooth (Fig 2-1) is largely composed of dentine, with a coronal enamel cap and a thin layer of cementum over the root. Enamel is the most radiopaque naturally occurring substance in the body, being about 90% mineral in composition. Thus, it can be differentiated from dentine (about 75% mineral). Cementum has a similar radiopacity to dentine and this, along with its thinness, means that it is not normally identifiable on radiographs.
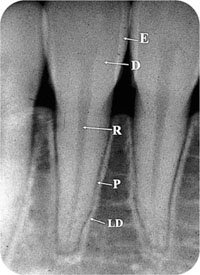
Fig 2-1 Periapical radiograph of a tooth. Cementum layers the root surfaces, but cannot be normally distinguished from dentine. E, enamel; D, dentine; P, pulp; R, root canal; P, periodontal ligament; LD, lamina dura.
The periodontal ligament is radiolucent relative to adjacent structures because it is principally made up of non-mineralised collagen. Its thickness varies even in health, but is typically 0.25–0.4 mm.
The lamina dura (lamina – “plate”; dura – “hard”) is a thin radiopaque thimble of dense bone that forms the tooth socket. Its radiopacity depends upon the thickness of lamina dura through which the x-ray beam passes. The radiopacity of the lamina dura and the radiolucency of the periodontal ligament will vary on radiographs from tooth to tooth and around different parts of the same tooth. Thus, the radiolucency of the ligament may appear greater (i.e. “darker”) where a greater depth of the ligament is in parallel alignment with the x-ray beam (Fig 2-2). This may lead to a subjective impression of ligament widening. The lamina dura may appear more prominent for the same reason.

Fig 2-2 On this periapical film, you can see that the periodontal ligament appears wider in some places (white arrows) than in others (black arrows). This reflects the depth of the ligament that is in parallel alignment with the x-ray beam.
Where roots have a more complex shape in cross-section – for example, on a lower permanent molar, a double periodontal ligament may appear, depending upon the direction of the x-ray beam incident upon the root (Fig 2-3). Furthermore, the two–dimensional image may mean that a periodontal ligament appears over the body of the tooth. This is often seen on upper molars, where the ligament space of the palatal root crosses over the mesiobuccal root (Fig 2-4).

Fig 2-3 “Double” periodontal ligaments on the roots of this lower molar.
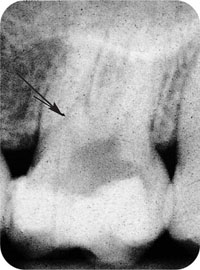
Fig 2-4 Periodontal ligament of the palatal root of 26 crossing the mesiobuccal root (arrowed).
Pulp anatomy
The anatomy of the coronal pulp and root canal system are particularly important to dentists in planning endodontic therapy. Pulp is radiolucent relative to surrounding dentine, but the degree of radiolucency varies according to the thickness of the pulp through which the x-ray beam passes. The apical foramen may sometimes be radiologically visible, emerging to the side of the root short of the radiographic apex in around 80% of roots. “Apical deltas”, where there is branching of the canal close to the apex, occur most commonly (10–15%) in maxillary second premolars and in both roots of mandibular first molars.
Vertucci extensively researched pulp anatomy of permanent teeth and described eight types of canal configuration:
Type I A single canal from pulp chamber to apex.
Type II Two canals leave the pulp chamber and join short of the apex.
Type III One canal leaves the pulp chamber, divides into two in the root and joins again before the apex.
Type IV Two distinct canals extend from pulp chamber to apex.
Type V One canal leaves pulp chamber and divides into two before the apex.
Type VI Two canals leave the pulp chamber, merge within the root but divide again before the apex.
Type VII One canal leaves the pulp chamber, divides and rejoins in the root and re-divides into two canals before the apex.
Type VIII Three distinct canals extend from pulp chamber to apex.
However, only four of these occur commonly (Fig 2-5). While this is a basic guide, lateral canals commonly arise from the root canal system and emerge on the side of the root. The details of the normal pulp anatomy types seen in the permanent dentition are as follows:
-
maxillary incisor and canine teeth have simple Type I pulp canal systems
-
the maxillary first premolar usually has a Type IV system, but about 18% have a Type II system
-
about half of maxillary second premolars have a single root with a Type I system, 22% have a Type II form, while 11% of teeth have a Type IV system. However, all forms are seen
-
the maxillary first permanent molar is a three-rooted tooth with a Type I canal system in the palatal and distobuccal roots. The mesiobuccal root is variable; surveys have shown that a significant minority have Type II or, less commonly, Type IV systems
-
the maxillary second permanent molar usually has three roots with Type I systems, but 17% have a mesiobuccal root with a Type II and 12% a Type IV form.
-
mandibular incisors have great variation in root canal morphology, meaning that additional radiographs employing parallax may be needed to illustrate it. The roots are wide labio-lingually and many have a dumbbell cross-sectional shape. About three quarters, however, have Type I canals. About 20% have Type III (Fig 2-6) and about 3% have Type IV canal systems
-
most mandibular canines are single-rooted with a Type I canal. However, a minority of teeth have Type II or Type IV systems
-
approximately 70% of mandibular first premolars have Type I canals, most of the remainder having Type V systems
-
almost all mandibular second premolars have Type I systems
-
the root canals of lower molars are very variable. 43% of mesial roots of the lower first molars have a Type IV system, with two separate canals. However, 28% of mesial roots have a Type II, 12% a Type I and 10% a Type VI system. Most (70%) distal roots of lower first molars have a Type I canal, with the remainder having various (II, IV, V, VI) types
-
although the lower second molar may follow the general morphology of the first molar, the mesial root has even greater variation in root canal anatomy, with all types seen. The distal root is most typically Type I.
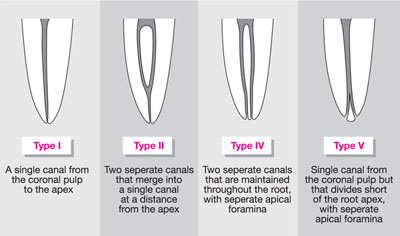
Fig 2-5 Principal types of pulp anatomy as defined by Vertucci in 1984. He described eight types (I-VIII), but only the four most common are shown here.
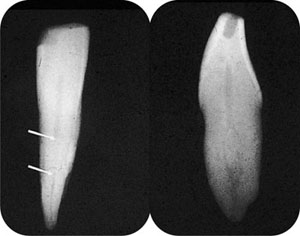
Fig 2-6 This extracted lower incisor tooth has a Type III canal system, splitting within the root and merging before the apex. The lateral image (right) reveals this, but examination of the conventional image shows that the canal becomes difficult to see (between the arrows), corresponding to where the split in the canal occurs.
The importance of obtaining optimal radiographic detail in endodontic diagnosis means that it is often advisable to obtain two periapical radiographs of a tooth to remove superimposition of canals and of canals upon periodontal ligaments. Apart from the example of lower incisors, the upper first molar is a good case of where two radiographs are helpful (Fig 2-7).

Fig 2-7 Parallax on upper first molar to separate roots and canals. On the first film (top) the palatal and mesiobuccal roots are superimposed. On the second film (bottom), the image has been produced by angling mesially, casting the mesiobuccal root away from the palatal root.
Pulp may contain variable amounts of calcification (see also Chapter 6). There are two types:
-
pulp stones
-
pulp sclerosis.
The former are discrete foci and the latter a more diffuse form of calcification, but may well be variants of the same process. Their frequency in the population, increasing with age, suggests that they may simply be a normal age change.
Pulp anatomy of deciduous teeth has many similarities with that of the permanent dentition. However, there are important differences:
-
thin prominent molar pulp horns
-
relatively large pulp chambers (and thinner surrounding dentine layer)
-
irregular ribbon-like canals
-
many small accessory canals in molars.
Developing Teeth
The earliest radiological sign of tooth development is a small radiolucency, the tooth crypt. This develops a thin radiopaque cortex at its periphery (Fig 2-8). The earliest calcification is in the developing incisal edge or cusp tips (Fig 2-9) of the tooth. This extends to form a radiopacity that begins to appear more recognisably “dental” in nature. The lamina dura persists around the crypt, forming a cap of bone ar/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


