2
Introduction to the dental surgery
A.S. Blinkhorn
Chapter contents
2.2 Psychology of child development
2.3 Parents and their influence on dental treatment
2.3.3 Should parents join children in the surgery?
2.3.4 Each patient is a unique individual
2.4 Dentist–patient relationship
2.4.1 People like friendly dentists
2.4.2 Structure of the dental consultation
2.5 Anxious and uncooperative children
2.6 Helping anxious patients to cope with dental care
2.6.5 Systematic desensitization
2.6.6 Hand over mouth exercise (HOME)
2.1 Introduction
It is a common belief among many individuals that being ‘good with people’ is an inborn art and owes little to science or training. It is true that some individuals have a more open disposition and can relate well to others (Fig. 2.1). However, there is no logical reason why all of us shouldn’t be able to put young patients at their ease and show that we are interested in their problems.
It is particularly important for dentists to learn how to help people relax, as failure to empathize and communicate will result in disappointed patients and an unsuccessful practising career. Communicating effectively with children is of great value, as ‘being good with younger patients’ is a practice-builder and can reduce the stress involved when offering clinical care.

Figure 2.1 Being good with patients is not necessarily an inborn art! (With thanks to David Myers and kind permission of Eden Bianchi Press.)
All undergraduate and postgraduate dental training should include a thorough understanding of how children relate to an adult world, how the dental visit should be structured, and what strategies are available to help children cope with their apprehension about dental procedures. This chapter will consider these items, beginning with a discussion on the theories of psychological development and following this up with sections on parents and their influence on dental treatment, dentist–patient relationships, anxious and uncooperative children, and helping anxious patients to cope with dental care.
2.2 Psychology of child development
At one time the psychological development of children was split into a series of well-defined phases, but more recently this division has been criticized and development should now be seen as a continuum. The phases of development may well differ from child to child, so a rigidly applied definition will be artificial. Nevertheless, for clarity when describing a child’s psychological development from infancy to adulthood, certain developmental milestones should be considered.
Academic considerations about psychological development have been dominated by a number of internationally known authorities who have, for the most part, concentrated on different aspects of the systematic progression from child to adult. However, the most important theoretical perspective now influencing thinking about child development is that of attachment theory—a theory developed by the psychoanalyst John Bowlby. In a series of writings over three decades, Bowlby developed his theory that child development could best be understood within the framework of patterns of interaction between the infant and the primary caregiver. If there were problems in this interaction, the child was likely to develop insecure and/or anxious patterns that would affect the ability to form stable relationships with others, to develop a sense of self-worth, and to move towards independence. The other important concept to note is that development is a lifelong process—we do not switch off at 18—nor is it an even process. Development is uneven, influenced by periods of rapid bodily change.
The psychological literature contains many accounts of the changes accompanying development. Therefore a general outline of the major ‘psychological signposts’ of which the dental team should be aware is presented in this section. As the newborn child is not a ‘common’ visitor to the dental surgery, no specific description of newborn behaviour will be offered; instead, general accounts of motor, cognitive, perceptual, and social development from birth to adolescence will be included. It is important to understand that the thinking about child development has become less certain and simplistic in its approach; hence dentists who make hard and fast rules about the way they offer care to children will cause stress to both their patients and themselves.
2.2.1 Motor development
A newborn child does not have an extensive range of movements, but these develop rapidly and by the age of 2 years the majority of children are capable of walking on their own. The ‘motor milestones’ occur in a predictable order, and many of the tests used by paediatricians assess normal development in infancy in terms of motor skills. The predictability of early motor development suggests that it must be genetically programmed. Although this is true to some extent, there is evidence that the environment can influence motor development. This has led to a greater interest in the early diagnosis of motor problems so that remedial intervention can be offered. A good example of intervention is the help offered to Down syndrome babies, who have slow motor development. Specific programmes which focus on practising sensorimotor tasks can greatly accelerate motor development to almost normal levels.
Motor development is really completed in infancy; the changes which follow the walking milestone are refinements rather than the development of new skills. Eye–hand coordination gradually becomes more precise and elaborate with increasing experience. The dominance of one hand emerges at an early age and is usually linked to hemisphere dominance for language processing. The left hemisphere controls the right hand and the right hemisphere controls the left. However, whereas the majority of right-handed people appear to be strongly left-hemisphere dominant for language processing, only 20% of left-handed people have right hemisphere dominance for language processing. Some children with motor retardation may fail to show specific right or left manual dominance and will lack good coordination between the hands.
Children aged 6–7 years usually have sufficient coordination to brush their teeth reasonably well. Below that age many areas of the mouth will be missed and there is a tendency to swallow relatively large amounts of toothpaste; hence parental supervision of brushing is important.
2.2.2 Cognitive development
The cognitive capability of children changes radically from birth through to adulthood, and the process is divided into a number of stages for ease of description. A Swiss psychologist called Piaget formulated the ‘stages view’ of cognitive development on the basis of detailed observations of his own children, and suggested that children pass through four broad stages of cognitive development (Table 2.1).
Dogma bites the dust
These stages have been highlighted because of the importance of Piaget’s early work on cognitive development. However, an over-reliance on ‘dogma’ may well limit the development of a subject, and this was the case with cognitive development. Few scientists challenged Piaget’s findings and the field of infant perception became a rather sterile area for a number of years, but this changed with the work of Bowlby. Enormous developments in research since then have led to many doubts being raised about Piaget’s original interpretation of his data. He underestimated the thinking abilities of younger children, and there is evidence to show that not all preschool thinking is totally egocentric. (See Key Point 2.1.)
 Key Point 2.1
Key Point 2.1
Babies and children are not unfinished adults. They are able to create, learn, and explore.
2.2.3 Are adults sensible?
Of just as much interest is the modern view that not all adult thinking is logical; many of us are biased and illogical. This is a self-evident truth when one considers the arguments raised against water fluoridation!
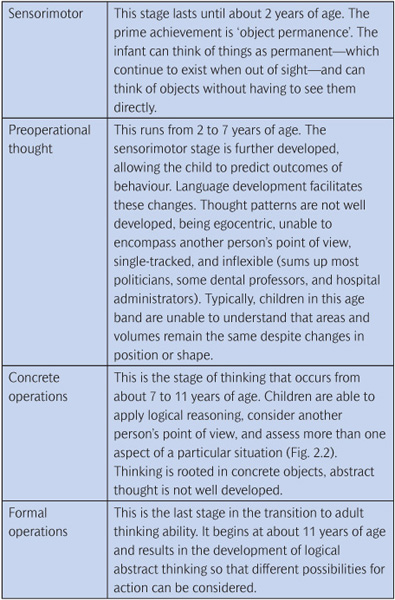

Figure 2.2 Children aged 7–11 years are able to consider another person’s point of view. (With thanks to David Myers and kind permission of Eden Bianchi Press.)
Figure 2.3 Be prepared for parents who don’t agree. (With thanks to David Myers and kind permission of Eden Bianchi Press.)
However, there is a serious point to this observation on adult illogicality. We must be prepared for parents who do not agree with our perceived wisdom (Fig. 2.3) or do not understand the basic tenets of specific programmes. Dentists will lead less stressful practising lives if they remember that not all their patients will always agree with or follow oral health advice.
So Piaget should be seen as a pioneer who really set in motion work on cognitive development, but it is now recognized that the developmental stages are not as clear-cut and many kids are smarter than we think!
2.2.4 Perceptual development
Clearly, it is very difficult to discover what babies and infants are experiencing perceptually; so much research has concentrated on eye movements. These types of studies have shown that with increasing age, scanning becomes broader and larger amounts of information are sought. Compared with adults, 6-year-old children cover less of the object, fixate on details, and gain less information. However, children do develop their selective attention, and by the age of 7 years can determine which messages merit attention and which can be ignored. Concentration skills also improve. Some dental advice can be offered to children of this age but, given the importance of the home environment, parents should be the main focus of any information given on oral healthcare.
With increasing age children become more efficient at discriminating between different visual patterns and reach adult proficiency by about 9 years of age.
The majority of perceptual development is a function of the growth of knowledge about the environment in which a child lives, hence the necessity to spend time explaining aspects of dental care to new child patients (Fig. 2.4).

Figure 2.4 Spend time explaining the facts about dental care. (With thanks to David Myers and kind permission of Eden Bianchi Press.)
2.2.5 Language development
A lack of appropriate stimulation will retard a child’s learning, particularly language. A child of 5 who can only speak in monosyllables and has no sensible sentence structure will not only be unable to communicate with others but also be unable to think about the things he/she sees and hears. Stimulation is important, as language development is such a rapid process in childhood that any delay can seriously handicap a child. Newborn children show a remarkable ability to distinguish speech sounds, and by the age of 5 years most children can use 2000 or more words. Language and thought are tied together and are important in cognitive development, but the complexities of the relationship between the two are not well understood.
Dentistry has a highly specialized vocabulary and it is unlikely that many children, or even adolescents, will understand our meaning if we rely on jargon. The key to successful communication is to pitch your advice and instructions at just the right level for different age groups of children. There is a risk of being patronizing if every child patient is told that ‘little pixies are eating away tiny bits of your tooth and I am going to run my little engine to frighten them away to fairyland’. A streetwise 10-year-old who is a computer games afficionado would probably call the police if you used such language! There is no universal approach to patients, so careful treatment planning and assessment are required before children or their parents are given specific written or verbal advice. (See Key Point 2.2.)
 Key Point 2.2
Key Point 2.2
Members of the dental team must assess children’s linguistic ability before offering advice. Tailor advice to individual families.
2.2.6 Social development
Until fairly recently it was believed that newborn infants were individuals who spent most of their time sleeping. However, recent research reveals that babies interact quite markedly with their environment, often initiating interactions with other humans by movement of their eyes or limbs.
Separation anxiety
Babies tend to form specific attachments to people and are prone to separation anxiety. At about 8 months infants show a definite fear of strangers. This potential for anxiety separation remains high until about 5 years of age, when separation anxiety declines quite markedly. This is consistent with studies of children in hospital, which show that after the age of 5 there is less distress on entering hospital. Separation anxiety should also be considered by dentists who insist that all young children must enter the dental surgery alone. Clearly, this will cause severe anxiety to patients under 5 years of age. (See Key Point 2.3.)
 Key Point 2.3
Key Point 2.3
Parents in the dental surgery cannot be governed by a rule. Each child and parent has different needs. A caring health professional should adopt some flexibility in his/her approach to offering clinical care with or without parents present.
It has been reported that a loving early parental attachment is associated with better social adjustment in later childhood and is a good basis for engendering trust and friendship with peers. This is important, as a successful transition from home to school depends on the ability to interact with other individuals apart from parents. The home environment will play a major part in social development, but the effects of community expectations should not be underestimated. We are all products of our broad social environment, mediated to some extent by parental influences.
2.2.7 Adolescence
The waning of parental influence can be seen in the final stage of child development—adolescence. This is the end of childhood and the beginning of adulthood. It is conceptualized as a period of emotional turmoil and a time of identity formation. This view is a Western creation and is culturally biased. In many societies ‘terrible teenagers’ do not exist; childhood ends and adult responsibilities are offered at a relatively early age.
It is interesting to note that even in Western industrialized societies there is little real evidence to support the idea that the majority of adolescents are rebellious and non-conformist. The main change is the evolution of a different sort of parental relationship. There is increasing independence and self-sufficiency. The research does show that young people tend to be moody, are oversensitive to criticism, and feel miserable for no apparent reason, but on the whole they do not rebel against their parental role models.
There are some clear messages to dentists who wish to retain their adolescent patients. Don’t criticize them excessively as this may compromise their future oral health. These patients are looking for support and reassurance. Many health professionals need to rethink their assumptions about young people, as personal behaviour patterns are not really related to health issues at all. Until there are acute problems ‘health per se’ is of little relevance to adolescents, being a rather abstract concept. Their major issues of concern are finding employment, exploring their sexuality, and having the friendship and support of their peers.
2.3 Parents and their influence on dental treatment
Children learn the basic aspects of everyday life from their parents. This process is termed socialization, and is ongoing and gradual. By the age of 4 years children know many of the conventions current in their culture, such as male and female roles. The process of transmitting cultural information early in life is called primary socialization. In industrialized countries, obtaining information on many aspects of life is gained formally in schools and colleges rather than from the family. This is termed secondary socialization.
2.3.1 Socialization
Interestingly, primary socialization can have a profound and lasting effect. For example, fear of dental treatment and when we first begin to clean our teeth can often be traced back to family influence, so parents can shape a child’s expectations and attitudes about oral health. Thus every attempt should be made to involve them when attempting to offer dental care or change a child’s health habits. (See Key Point 2.4.)
 Key Point 2.4
Key Point 2.4
Maintaining a healthy mouth begins in early childhood as the teeth erupt. It is far simpler to encourage healthy habits than to change ingrained behaviour.
2.3.2 Avoid victim blaming
Involving parents means that the dentist must look to positive reinforcement rather than ‘victim blaming’. Parents who are accused of oral neglect may well feel aggrieved or threatened. All too often children’s oral health is compromised by a lack of parental knowledge, so programmes have to be carefully designed to reduce any chances of making people feel guilty. Guilt often results in parents spending more time seeking excuses for problems than trying to implement solutions.
Parents who are convinced that their child has an oral health problem which can be solved tend to react in a positive way both to their dental advisor and to the preventive programme itself. It is especially helpful if the preventive strat/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


