Selective Grinding
“SELECTIVE GRINDING: ONE OF THE MOST DIFFICULT AND DEMANDING PROCEDURES IN DENTISTRY.”
—JPO
SELECTIVE GRINDING IS A PROCEDURE by which the occlusal surfaces of the teeth are precisely altered to improve the overall contact pattern. Tooth structure is selectively removed until the reshaped teeth make contact in such a manner as to fulfill the treatment goals. Since this procedure is irreversible and involves the removal of tooth structure, it is of limited usefulness. Therefore proper indications must exist before it is considered.
Indications
A selective grinding procedure can be used to (1) assist in managing certain temporomandibular disorders (TMDs) and (2) complement treatment associated with major occlusal changes.
Assistance in Managing Certain Temporomandibular Disorders
Selective grinding is indicated when sufficient evidence exists that permanent alteration of an occlusal condition will reduce or eliminate the symptoms associated with a specific TMD. This evidence cannot be determined by the severity of the malocclusion. As discussed in Chapter 7, the severity of the malocclusion does not correlate well with symptoms partly because of the great variation in patients’ physiologic tolerances and also because the malocclusion may not reflect orthopedic instability (a stable malocclusion). The evidence for the need to permanently change the occlusal condition is obtained through reversible occlusal therapy (e.g., occlusal appliance therapy). Selective grinding is indicated when (1) the occlusal appliance has eliminated the TMD symptoms and (2) attempts to identify the feature of the appliance that affects the symptoms have revealed that it is the occlusal contact or jaw position. When these conditions exist, it is likely that if the occlusal condition provided by the appliance were permanently introduced in the dentition the disorder would resolve. Then and only then is there significant confidence that selective grinding is indicated and would provide a level of success.
Complementing Treatment Associated with Major Occlusal Changes
The most common reason to considering selective grinding is as part of a treatment plan that will result in a major change in the existing occlusal condition. This reason for the treatment is not associated with a TMD but entails a significant restoration or reorganization of the occlusal condition. When major occlusal changes are planned, treatment goals should be established that will provide optimal occlusal conditions when the treatment is completed. If extensive crown and fixed prosthodontic procedures are necessary, selective grinding may be indicated before treatment begins so that a stable functional mandibular position is established to which the restorations can be fabricated.
In summary, selective grinding is indicated to improve an occlusal condition only when sufficient evidence exists that this alteration will assist in the management of a TMD or in conjunction with an already established need for major occlusal treatment. There is no evidence at present that prophylactic selective grinding is of benefit to the patient.
Predicting the Outcome of Selective Grinding
Even when alteration of the occlusal condition is indicated, a selective grinding procedure may not be the treatment of choice. Selective grinding is appropriate only when alterations of the tooth surfaces are minimal so that all corrections can be made within the enamel structure. When the misalignment of teeth is great enough that achieving the treatment goals will penetrate the enamel, selective grinding must be accompanied by proper restorative procedures. Exposure of dentin poses problems (increased sensitivity, caries susceptibility, and wear) and therefore should not be left untreated. It is extremely important that the treatment outcome of selective grinding be accurately predicted before treatment begins. Both the operator and the patient must know and be prepared in advance for the results of the selective grinding procedure. Patient acceptance and rapport are not strengthened when, after the procedure is completed, additional crowns necessary to restore the dentition are added to the treatment plan.
The success in achieving the treatment goals using a selective grinding procedure alone is determined by the degree of misalignment of the teeth. Since it is necessary to work within the confines of the enamel, only minimal corrections can be made. The “rule of thirds” (Chapter 17) is helpful in predicting the success of a selective grinding procedure. It deals with the buccolingual arch discrepancy when the condyles are in the musculoskeletally stable position (Figure 19-1).

The anteroposterior discrepancy must also be considered. It is best examined by visualizing the centric relation–to–intercuspal position (CR-to-ICP) slide, which is observed by locating the mandible in the musculoskeletally stable position (CR) and with a hinge axis movement bringing the teeth into light contact. Once the buccolingual discrepancy of the posterior teeth is examined (rule of thirds), the patient applies force to the teeth. An anterosuperior shift of the mandible from CR to the ICP will be noted. The shorter the slide, the more likely it is that selective grinding can be accomplished within the confines of the enamel. Generally an anterior slide of less than 2 mm can be successfully eliminated by a selective grinding procedure.
The direction of the slide in the sagittal plane can also influence the success or failure of selective grinding. Both the horizontal and the vertical components of the slide should be examined. Generally when the slide has a great horizontal component, it is more difficult to eliminate within the confines of the enamel (Figure 19-2). If it is almost parallel with the arc of closure (large vertical component), eliminating it is usually easier. Therefore both the distance and the direction of the slide are helpful in predicting the outcome of selective grinding.
After the CR slide has been examined, the position of the anterior teeth is evaluated. These teeth are important, since they will be utilized to disocclude the posterior teeth during eccentric movements. With the condyles in their treatment position (CR), the mandible is once again closed until the first tooth contacts lightly. An attempt is made to visualize the relationship of the maxillary and mandibular anterior teeth as if the arc of closure were continuing until the patient’s vertical dimension of occlusion were achieved. This represents the position of the anterior teeth after the premature CR contacts have been eliminated. An attempt is made to predict the type and adequacy of the future anterior guidance.
It is relatively easy to predict the treatment outcome in a patient with well-aligned teeth and a very short CR slide. It is equally easy to determine that a patient with a 6-mm horizontal slide and poorly aligned teeth is not a good candidate for this procedure alone. The problem with predicting the outcome of selective grinding arises with the patient who is between these two extremes. Therefore, when it is difficult to determine the outcome of selective grinding, accurate diagnostic casts are carefully mounted on an articulator so that further analysis can be made. Tooth alignment and the CR slide are more easily evaluated on mounted diagnostic casts. When doubt still exists, selective grinding is carefully performed on the diagnostic casts so the final results can be visualized. Teeth that are severely altered should be planned for crowns. Once the results of the selective grinding are visualized, the potential benefits of the procedure can be weighed against any additional treatment needed to restore the dentition. These considerations must be evaluated before a selective grinding procedure is suggested to the patient.
Important Considerations in Selective Grinding
After the determination has been made that there are proper indications for selective grinding and treatment results have been adequately predicted, the procedure can begin. It is advisable, however, not to rush into treatment without thoroughly explaining the procedure to the patient. In some cases the success or failure of the treatment will hinge on the acceptance and assistance of the patient. It should be explained that there are very small areas of the teeth that interfere with the normal functioning of the jaw and that the goal is to eliminate these so that normal function can be restored. The patient should be aware that although such a procedure may take some time, the changes are very slight and often difficult to visualize in the mirror. Any questions regarding the procedure should be discussed and explained before the procedure begins. The treatment outcome must be thoroughly explained, especially if any restorative procedures will be necessary.
From the technical point of view, selective grinding can be a difficult and tedious procedure. It should not be initiated haphazardly or without a complete understanding of the treatment goals. A well-performed selective grinding procedure will enhance function of the masticatory system. On the other hand, a poorly performed one may actually create problems with masticatory function and even accentuate occlusal interferences that have been previously overlooked by the neuromuscular system (creating what has been called a positive occlusal awareness). It may therefore initiate functional problems. A well-executed selective grinding procedure does not lead to positive occlusal awareness. Rather, the condition usually occurs in patients with high levels of emotional stress or other emotional problems such as obsessive compulsive behavior disorders. Such problems are best avoided by, first, being sure that there are proper indications for selective grinding (emotional stress is not a major factor) and, second, carrying out the procedure carefully and precisely.
The effectiveness of selective grinding can be greatly influenced by the operator’s ability to manage the patient. Since the procedure demands precision, careful control of the mandibular position and tooth contacts is essential. The patient’s muscular activity must be properly restrained during the procedure so that the treatment goals can be accomplished. Therefore conditions that exist during the procedure should promote patient relaxation. Selective grinding is performed in a quiet and peaceful setting. The patient is reclined in the dental chair and approached in a soft, gentle, understanding manner. Encouragement is given when success in relaxing and aiding the operator is achieved. When it is advantageous for the operator to guide the mandible to a desired position, the movement is performed slowly and deliberately so as not to elicit protective muscle activity. The success of a selective grinding procedure is dependent on all these considerations.
Treatment Goals of Selective Grinding
Although selective grinding involves the reshaping of teeth, the mandibular position to which the teeth are altered is also critical. Selective grinding should begin with locating the musculoskeletally stable (CR) position of the condyles. This is done using the bimanual manipulation technique described in Chapter 9. In the patient with a TMD an occlusal appliance may have been used to help determine the stable joint position. If for any reason the condylar position is in question, selective grinding should not be initiated until a stable, reproducible position has been achieved.
The occlusal treatment goals of selective grinding are as follows:
Several methods can be used to achieve these goals. The one described here consists of developing, first, an acceptable centric relation contact position and, second, an acceptable laterotrusive and protrusive guidance.
Developing an Acceptable Centric Relation Contact Position
The goal of this step is to create desirable tooth contacts when the condyles are in their musculoskeletally stable (CR) position. In many patients an unstable occlusal condition exists in CR and creates a slide to the more stable ICP. A major goal of selective grinding is to develop a stable intercuspal contact position when the condyles are in the CR position.
Another way of describing this goal is to refer to it as elimination of the centric relation slide. A slide of the mandible is created by the instability of contacts between opposing tooth inclines. When the cusp tip contacts a flat surface in centric relation and force is applied by the elevator muscles, no shift occurs. Thus the goal in achieving acceptable contacts in ICP is to alter or reshape all inclines into either cusp tips or flat surfaces. Contacts from cusp tip to flat surface are also desirable since they effectively direct occlusal forces through the long axes of the teeth (Chapter 5).
The CR slide can be classified as anterosuperior, anterosuperior and to the right, or anterosuperior and to the left. Each is created by specific opposing inclines. A basic understanding of these makes establishing an acceptable CR position much simpler.
Anterosuperior slide
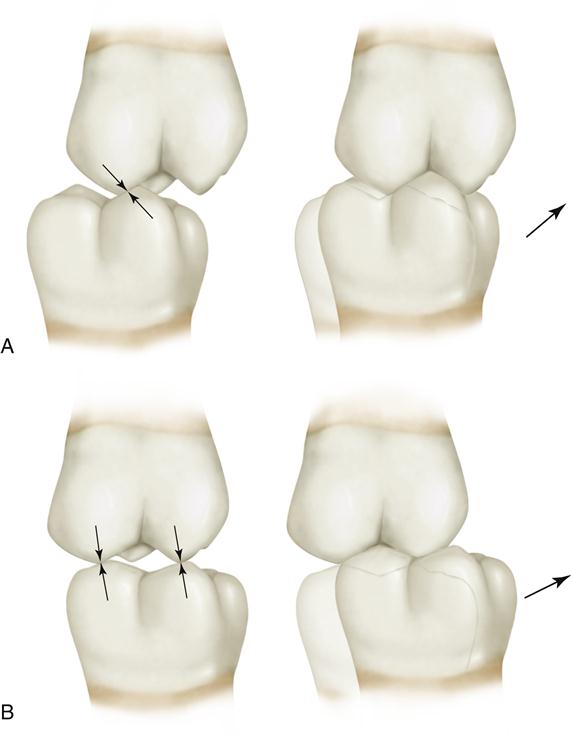
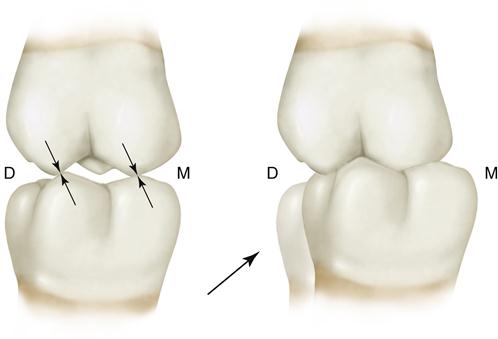
The slide from CR to maximum intercuspation may follow a pathway that is straightforward and superior in the sagittal plane. It is due to contact between the mesial inclines of the maxillary cusps and the distal inclines of the mandibular cusps (Figure 19-3).
Anterosuperior and right slide
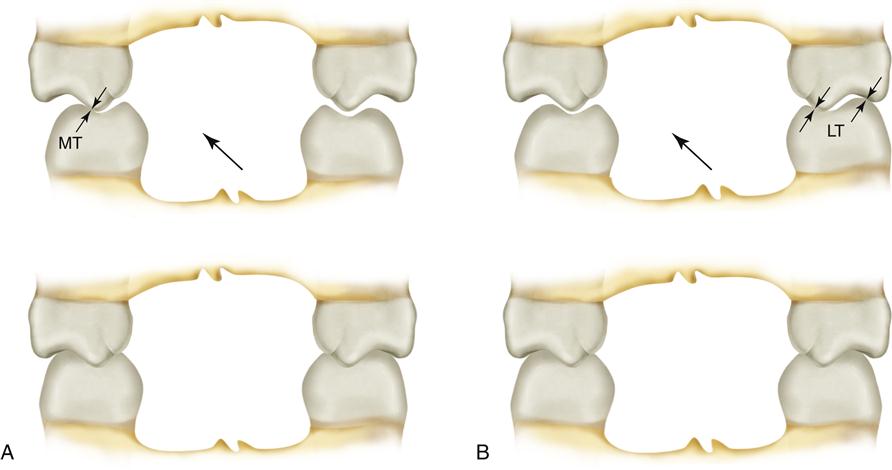
The CR slide may be anterosuperior with a right lateral component (i.e., moving to the right). When there is a lateral component, it is due to the inner and outer inclines of the posterior teeth.
When a right lateral slide is created by opposing tooth contacts on the right side of the arch, it is due to the inner inclines of the maxillary lingual cusps against the inner inclines of the mandibular buccal cusps. Since these are also the locations for mediotrusive contacts, they are sometimes called mediotrusive CR interferences (Figure 19-4, A).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


