17
Occlusion: Adjustment and Splints
After analysing the occlusion by performing a clinical examination and laboratory assessment, the next step is deciding whether any occlusal adjustment or occlusal splints are necessary before starting prosthodontic therapy.
Occlusal Adjustment
Occlusal stabilisation by occlusal adjustment (OA) is a controversial topic. Before discussing opposing theories, if TMD (temporomandibular disorder) is suspected, differential diagnosis is essential to elucidate whether TMD symptoms originate due to myogenous or bruxism origins, or pathology of the mandibular articular region. If the latter is suspected, occlusal adjustment is futile.
However, if TMD problems originate from myogenous or bruxism causes, OA may or may not alleviate symptoms. There are two schools of thought regarding OA. The first states that neuromuscular feedback will adapt to any adjustments and therefore negate its effect. The second opinion is that OA can stabilise the occlusion, removing interferences that impede physiological mandibular excursions, and hence provide symptomatic relief. Whichever opinion one holds, in order to prevent irreversible occlusal destruction, it is probably prudent to avoid OA until further conclusive research is forthcoming.
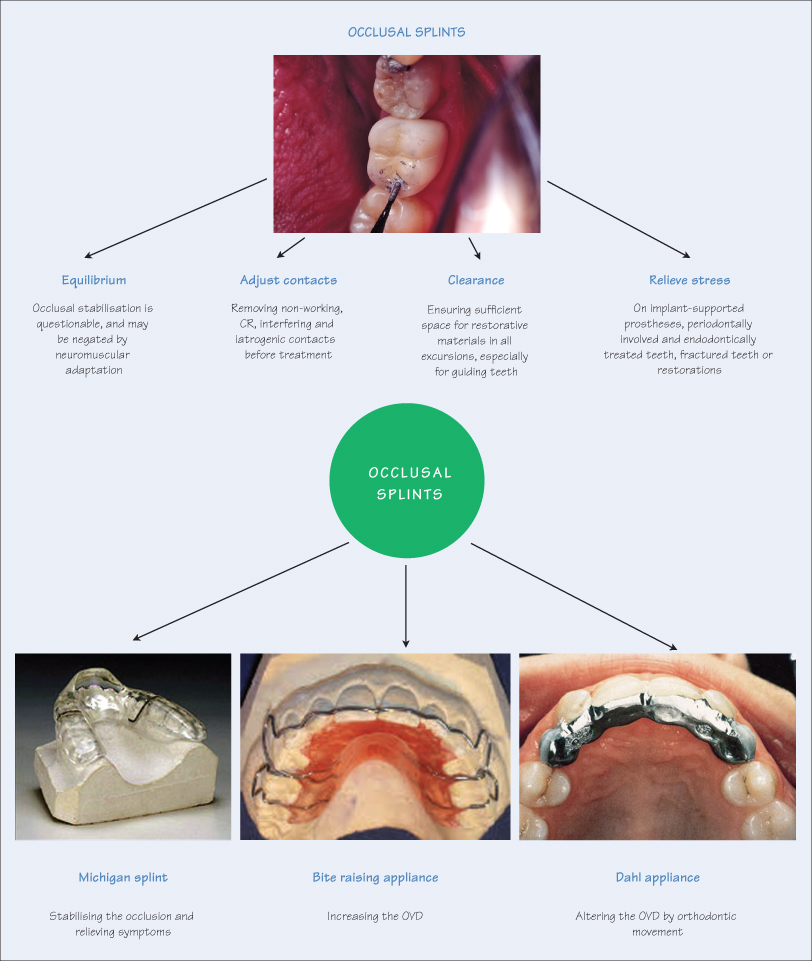
Besides TMD reasons, selective OA is justified before starting restorative treatment. Preoperative adjustments can be invaluable in saving time and avoiding disappointment as treatment progresses, especially at the cementation stage to ‘grind in’ the restoration(s), for example:
- Removing non-working side interferences causing lifting of the mandible on the working side;
- Ensuring sufficient occlusal clearance for restorative materials in all excursions (particularly for guiding teeth);
- If the tooth to be restored is the initial contact />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


