Traumatology
Classification
Various classification systems have been proposed over the years, including those by Ellis (1945), WHO (1978, 1992), and Andreasen and Andreasen (1992). It is important to refer to a complete and easy-to-use classification system that permits simple identification of the type of lesion that can be encountered in daily practice. The description of dental trauma and related clinical cases presented in this chapter refers to the classification of dental trauma proposed in 1988 by Spinas-Piroddi and approved by the Italian Society of Traumatology (JADT).
Effects of trauma on the tissues
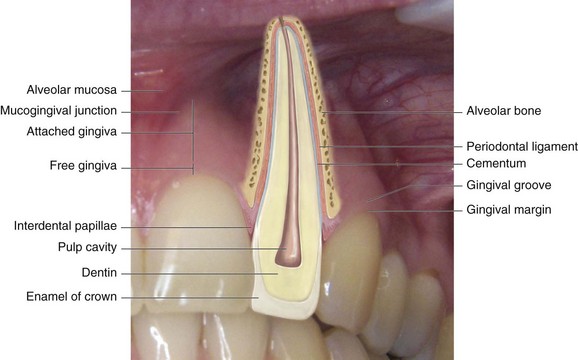
Dentoalveolar traumatic injuries affect many tissues and structures, and the lesion of the affected structures determines the resulting damages. Any prognosis—regardless of whether it is functional or esthetic or involves the pulp and the permanence of the tooth in the oral cavity—requires knowledge of the normal configuration of the tooth and its supporting tissues (Figure 15-1).
Treatment
Crown Fractures
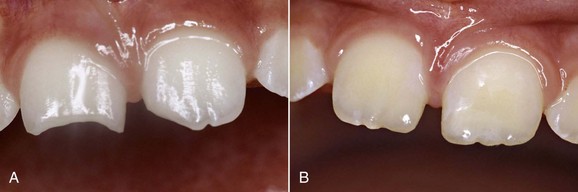
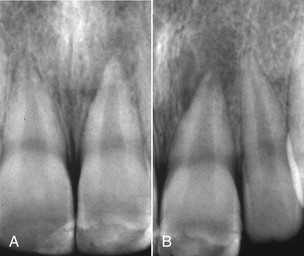
In the case of class A, B, and C coronal fractures (Figures 15-2, 15-3, and 15-4) according to the Spinas-Piroddi classification, treatment involves composite restoration or reattachment of the original fragment when found. Class B1 and C1 coronal fractures (Figures 15-5 to 15-10) likewise require composite restoration or reattachment of the original fragment when found. If root formation is not complete, the treatment entails pulp capping, whereas if the pulp is necrotic the tooth must be treated endodontically. When the pulp is necrotic but the apex is immature, apexification of the root must be induced. Class D and D1 fractures (Figures 15-11 to 15-14) require composite restoration or reattachment of the recovered tooth fragment. If root involvement extends below the alveolar ridge, the treatment requires a clinical crown-lengthening procedure or orthodontic extrusion. If the pulp is affected, the dentist must evaluate whether the tooth should undergo endodontic treatment or a pulp capping procedure.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


