chapter 15 Inhalation Sedation: Techniques of Administration
The administration of nitrous oxide-oxygen (N2O-O2) for pharmacosedation is a very easy and straightforward procedure. It requires an approved sedation unit, a trained administrator, and a patient desiring sedation. Proper training conveys confidence to the patient and, as a result, an expectation of a successful outcome. Training, as defined by the American Dental Association guidelines, requires instruction in pain and anxiety control consisting of 14 hours of course content, including a clinical component during which competency in inhalation sedation technique is achieved.1 Even though N2O-O2 is considered a very safe drug, a number of unpleasant and potentially dangerous complications can still develop. Therefore the person responsible for the administration of N2O-O2 must be aware of these potential problems; know how to prevent them from occurring and how to recognize and manage them.
GENERAL DESCRIPTION
The technique of inhalation sedation for the cooperative adult patient (an apprehensive patient who willingly accepts the nasal hood) is as follows. Management of the more difficult patient, such as the child or adult with a disability or the pediatric patient, is described in Chapters 35 and 38.
ADMINISTRATION
Day of Appointment
Monitoring During Inhalation Sedation
The following is the recommended monitoring for inhalation sedation procedures:
Preparation of the Equipment
Experts in the use of N2O-O2 met in 1995 at the request of the American Dental Association to consider the then-current use of N2O-O2 in the dental office.2 One outgrowth of that meeting was the development of guidelines for equipment inspection and use. They are as follows.
Preparation of the Patient
Technique of Administration
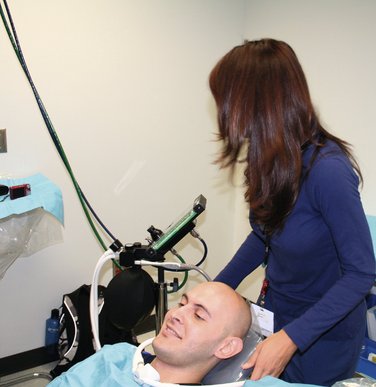
COMMENT: The preferred position (Figure 15-1) is first a consideration of patient comfort. The partially reclined position may be used, if necessary, for the patient’s comfort or the convenience of the dentist during the procedure. The upright position is not recommended unless essential for the procedure, such as when taking impressions or radiographs.

COMMENT: This procedure applies only to the use of the portable inhalation sedation unit (Figure 15-2), as opposed to the fixed, central systems commonly found in dental offices. The N2O-O2 unit should always be placed behind the patient, out of his or her line of sight. A positive placebo response will occur in a some patients receiving N2O-O2, but if the patient can see the unit and watch as the administrator adjusts the controls, this response can be negated.
COMMENT: Placing the nasal hood on the patient (Figure 15-3) after starting the flow of O2 will prevent the patient from feeling suffocated when breathing through the nose if the O2 flow is not begun before placement of the nasal hood.

COMMENT: The nasal hood usually has two hoses coming from the N2O-O2 unit. These are placed around the sides of the dental chair, and the nasal hood is secured by adjusting the slip ring behind the headrest (Figure 15-4). The patient is asked to hold the nasal hood in a comfortable position as this is done. Care must be taken in adjusting the nasal hood because one of the tubes is often pulled more than the other, making the nasal hood tilt to one side.

Leaks develop on occasion around an ill-fitting mask. Nasal hoods are available in a variety of sizes. The size is checked before the start of the procedure. The nasal hood used should fit the patient’s nose. An overly small or overly large mask will leak. Leaks may also develop with masks of the appropriate size. Most often, these leaks occur around the bridge of the nose, with the patient complaining of “air” exhaled into his or her eyes. Permitting the patient to adjust the nasal hood is often all that is needed to correct this situation. If this simple solution is ineffective, the hood is removed, a folded 2-inch square gauze pad is placed over the bridge of the nose, and the nasal hood is replaced. This usually seals the leak (Figure 15-5).

When a scavenging nasal hood (recommended) is used, the exhalation tubes must be connected to the vacuum system. It is important to adjust the vacuum so that the patient is able to exhale and inhale comfortably.2 If the vacuum is too weak, the patient may experience difficulty in breathing out, and if the vacuum is too forceful, the patient may not receive any N2O-O2 because the gases are rapidly sucked from the nasal hood into the overly efficient vacuum system.
Establishing the minimal flow rate is important because if it is assumed that the patient can tolerate 6 L/min comfortably but actually cannot, then the individual will probably never become comfortably sedated with N2O-O2 during the procedure. This step is always carried out with the patient receiving 100% O2 (Figure 15-6).
The reservoir bag that remains partially inflated (deflated) (Figure 15-7, A) and deflates and inflates partially with each breath usually indicates that the minute volume is adequate (the bag remains partially inflated throughout the procedure) and that the seal of the nasal hood is tight (inflates and deflates with each breath).



A bag that remains totally deflated (Figure 15-7, B) may indicate one of the following:
A bag that is overly inflated (Figure 15-7, C), looking like a balloon about to burst, may indicate one of the following:
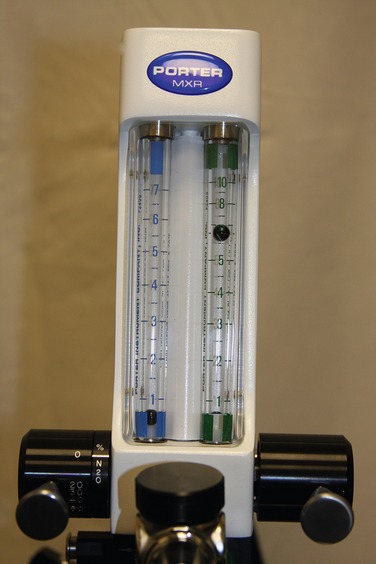
When operating a unit with individual control knobs for N2O and O2 and using the constant liter flow technique, the administrator increases the N2O flow to 1 L/min and then decreases the O2 flow rate to 5 L/min (Figure 15-8). This produces an N2O percentage of 16.6% (1 L/min N2O/6 L/min total gas flow). In the constant O2 flow technique, the O2 flow is left at its initial rate (6 L/min in this case) and the N2O flow is increased to 1 L/min. The N2O concentration is 14.3% (Figure 15-9).
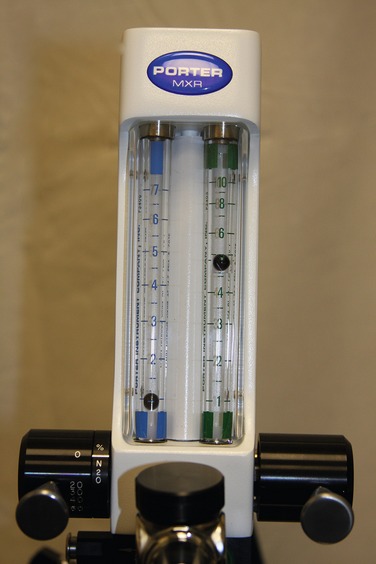



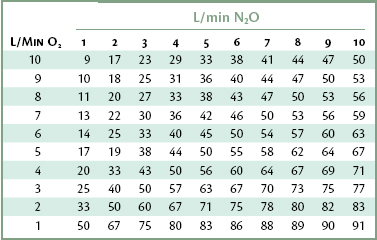
Table 15-1 provides an easy method of determining the percentage of N2O delivered at common flow rates.
Two points that may appear minor must be mentioned:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


