Notes on Pediatric Dentistry
Caries and Caries Prevention
Even in the earliest months of life some children need dental care and procedures for early caries, attributable to the incorrect use of baby bottles containing sweetened drinks. Chamomile or sweetened herbal teas are often given to children to relieve the pain of infant colic at night. This can lead to a condition known as early childhood caries (ECC) or baby bottle tooth decay (BBTD) (Figure 14-1).

Etiopathogenesis
Caries is a transmissible infectious disease of bacterial origin. It is one of the most widespread diseases in the world. The most common chronic infection in childhood, it is 5 times more frequent than fever and 14 times more common than chronic bronchitis (Evans and Kleinman, 2000). It affects the following populations:
In Italy the percentages are lower:
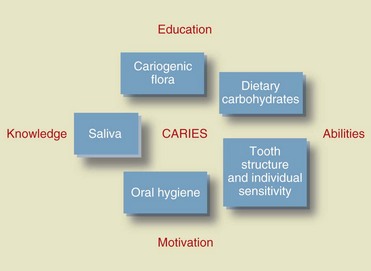
Caries has a multifactorial etiology: bacterial flora, host susceptibility, diet, and the time factor play key roles in the development of lesions (Figure 14-2). The carious process consists of the acid dissolution of the tooth structure.
The Stephan curve represents the lowering of pH and its subsequent rise after the introduction of sugar in the mouth over a period of about 1 hour (Figures 14-3 and 14-4).
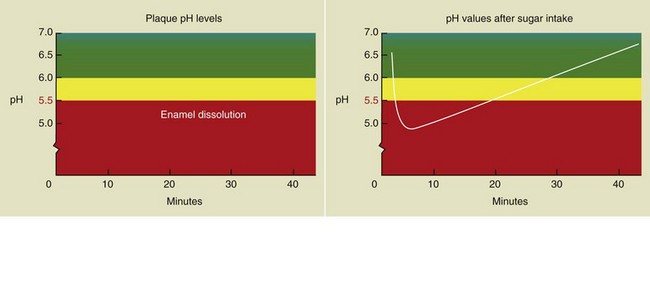
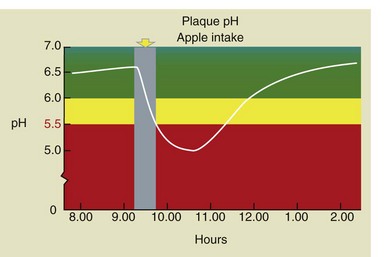
Figure 14-4 The Stephan curve changes after an apple is eaten. In this case the pH is lowered for a short time.
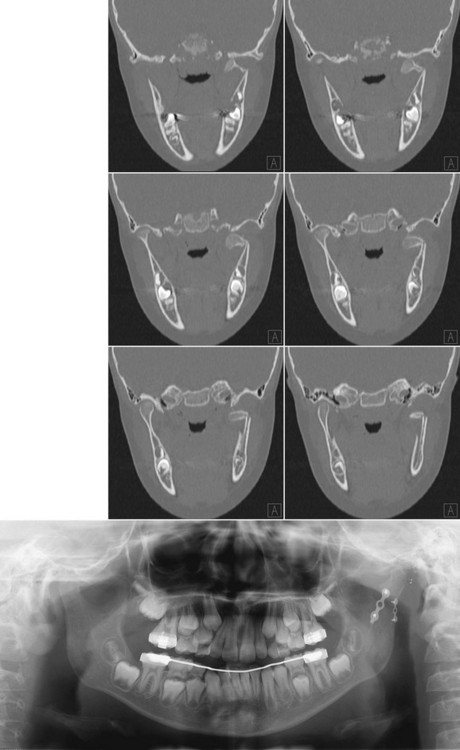
When a child exhibits carious lesions during the first years of life, ECC can be diagnosed based on the following typical signs of the disease (European Journal of Paediatric Dentistry, 2004) (Figure 14-5):

Figure 14-5 Diagram of mother-infant bacterial infection.
• Rapid development occurs: enamel-dentin progression is less than 6 months.
• The upper incisors are the first teeth to be affected.
• Subsequently the first upper and lower molars are affected.
• In the final stages, when the disease is very severe and has gone untreated, the lower incisors are also affected.
The objectives established by WHO for the year 2010 were as follows:
Preventive Measures
Deciduous Dentition
Moreover, many foods and beverages also contain fluoride. Therefore systemic fluoride prophylaxis must take all sources of intake into account (Box 14-1).
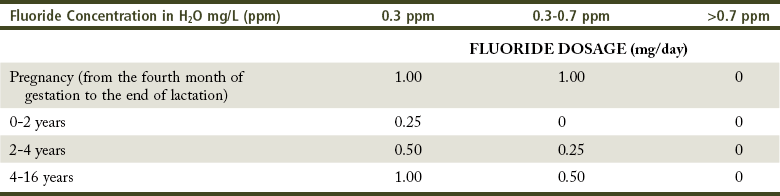
After 4 years of age the use of fluoride gel can be recommended for children at medium to high risk for caries who are able to swallow (Tables 14-1 and 14-2).
TABLE 14-1
Summary of Fluoride Prophylaxis Based on the Concentration of Fluoride in Water*
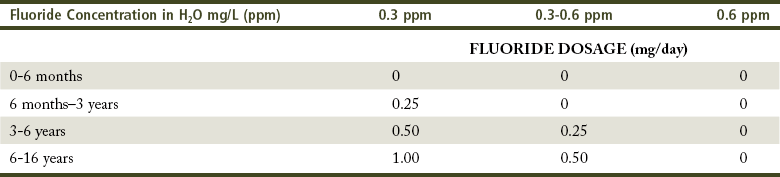
*American Academy of Pediatric Dentistry and European Academy of Paediatric Dentistry (AAPD/EAPD), 1994.
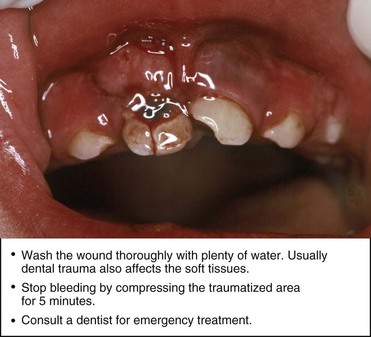
It is important to note that the pediatrician is the one who takes care of prevention from birth. Therefore, he or she can be considered the most important point of reference for both children and parents. When there is an emergency, the pediatrician works with the dentist to inform the parents and caregivers about the correct measures to take. The pediatrician will provide guidance on how to practice first aid, stressing the importance of adequate follow-up to avoid long-term complications (Figure 14-6).
Deciduous tooth shedding begins around 5 years of age, but timing and eruption mechanisms may vary.
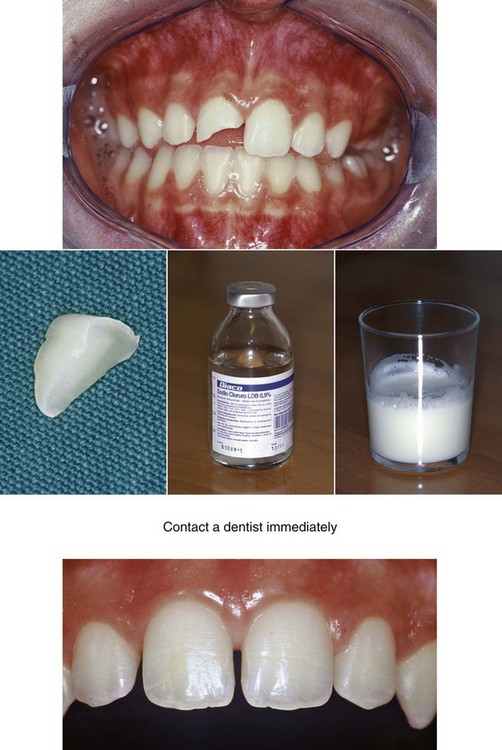
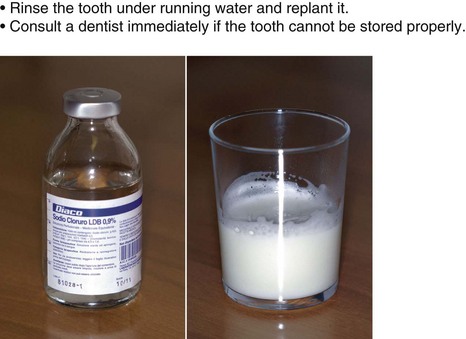
In addition to injuries that can occur at school and during play or sports activities, we must also consider those caused by bicycle falls (Figures 14-7 to 14-9).
Permanent Dentition
Fluoride and sealants are currently the most effective protective measures against caries (Figure 14-10). Patients with high caries risk should be treated with preventive sealing of pits and fissures of the first permanent molars (Figure 14-11).
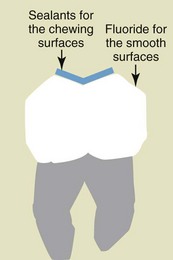
Figure 14-10 Sealants and fluoride protection against caries.

Figure 14-11 Sealing of a first permanent molar.
At 8 years of age the child should be able to perform oral hygiene practices autonomously, understand the importance of regular dental checkups, and learn to communicate directly with the dentist. Proper oral health education that starts in the earliest years of life can positively influence the child’s perception of the dentist and the dental environment (Figure 14-12).
Figure 14-12 A child’s drawing of the dental office.
When the permanent incisors erupt (Figure 14-13) they may show signs of fluorosis, particularly in children who have used naturally fluoridated water and those in whom fluoride prophylaxis was administered overenthusiastically (Figure 14-14). It is important to exclude all other causes of enamel alteration, such as celiac disease, trauma to the deciduous dentition, and structural abnormalities that are genetic and pharmacologic in nature.
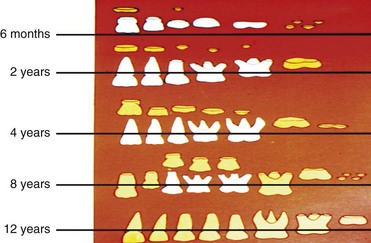

Figure 14-14 Signs of fluorosis in a young patient.
For patients at high risk for caries, sealing of the second molars may also be indicated.
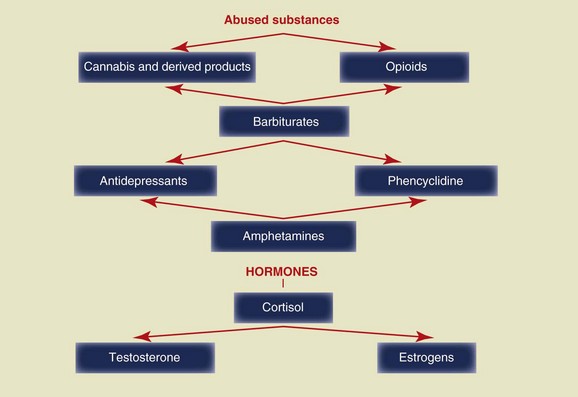
Given the unquestionable effectiveness of prevention, as early as the age of 10 children should be informed about the consequences of the abuse of certain substances on the oral cavity (Figure 14-15).
By age 16, deciduous tooth shedding has already been completed for some time and the dentition is relatively stable. Therefore attention must paid to third molars, and their presence and the space available for their eruption should be checked. At this point the orthodontist will evaluate the timing and possible need for extraction (Figure 14-16).

Food
Carbonated drinks often contain large amounts of caffeine, which—along with sugar—can cause a significant increase in the incidence of caries (Table 14-3).
TABLE 14-3
Concentration of Caffeine (mg) in Commonly Consumed Foods and Beverages
| Coffee | 100-140 mg |
| Tea | 25-40 mg |
| Iced tea | 20-50 mg |
| Cola drinks | 34-45 mg |
| Noncarbonated cola drinks | 40-55 mg |
| Caffeinated water | 45-90 mg |
| Chocolate milk | 20-50 mg |
| Chocolate bars | 25-35 mg |
From American Academy of Pediatric Dentistry.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


