13
Behavior Management in Dentistry: Thumb Sucking
- Thumb sucking, common in young children, often causes dental problems when it persists for years.
- Thumb sucking persists in most cases because it modulates arousal or provides sensory stimulation.
- Successful treatments must work in the absence of the parent as thumb sucking often occurs when the child is alone.
- Successful treatments involve response prevention, management of covarying behaviors, consequence procedures, and combination procedures.
Thumb and finger sucking (hereafter called thumb sucking) is common in early childhood. Studies of the prevalence of thumb sucking show that one quarter to one half of children aged 3–6 years suck their thumbs (e.g., Troster, 1994; Widmalm, Christiansen, & Gunn, 1995; Gutermuth-Foster, 1998). Interestingly, studies conducted in other countries have shown that the prevalence of thumb sucking is substantially lower (e.g., Vignarajah & Williams, 1992; Kharbanda et al., 2003), suggesting that thumb sucking may be influenced by cultural practices.
Although there is very little empirical support for the notion that thumb sucking is symptomatic of psychological disturbance or psychopathology in children (e.g., Tryon, 1968; Friman, Larzelere, & Finney, 1994), a number of physical problems are correlated with thumb sucking if it persists beyond the age of 4 or 5 years. Thumb sucking may contribute to malocclusion (e.g., Reid & Price, 1984; Afzelius-Alm et al., 2004), digital deformities (e.g., Reid & Price, 1984; Rankin et al., 1988; Malek, Oger, & Rivet-Forsans, 1994), temporomandibular disorders (e.g., Widmalm et al., 1995; Sari & Sonmez, 2002), altered facial-muscle activity (Ahlgren, 1995), and increased susceptibility to toxins (e.g., Cowie, Black, & Fraser, 1997). In addition to physical problems, Friman et al. (1993) found that first graders who engaged in thumb sucking received lower ratings of social acceptance from their non-thumb-sucking peers. Thus, children who continue to suck their thumb beyond the age of 4 years may require behavioral intervention. This chapter discusses behavioral assessment and intervention for thumb sucking.
Assessment of Thumb Sucking
Behavioral assessment of thumb sucking is necessary to document the severity of the problem and to evaluate the effects of treatment. Behavioral assessment will involve direct observation and recording of the behavior as it occurs in the child’s natural environment. To make assessment most valid, observations should be conducted at the time and in the location the child is most likely to engage in thumb sucking.
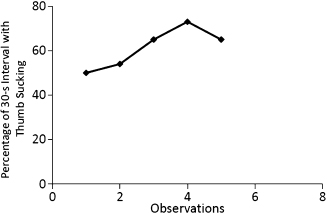
Because the length of time the thumb is in the child’s mouth is the most important aspect of the behavior, a duration measure often is chosen for recording thumb sucking. Duration events typically are measured in one of two ways. An observer can record the total number of seconds during an observation period for which a child engages in thumb sucking. This approach is often referred to as continuous duration recording (CDR; Rapp et al., 2007). When using CDR, an observer records the length of time thumb sucking is observed throughout the designated observation period and then reports the percentage of time for which the behavior occurred (duration of thumb sucking divided by the duration of the observation period; Long, Miltenberger, & Rapp, 1999b; Rapp et al., 1999). Alternatively, when CDR is viewed as too effortful or time-consuming, an observer can utilize discontinuous recording methods such as momentary time sampling (MTS). Although discontinuous methods are less sensitive for detecting changes in thumb sucking produced by intervention, a number of studies have shown that MTS with interval sizes up to 30 seconds can detect a high proportion of meaningful changes in duration events (Meany-Daboul et al., 2007; Rapp et al., 2007, 2008; Devine et al., 2011). When using MTS with 30-second intervals, the observer divides the observation period into consecutive 30-second bins and designates 1 second in each bin (typically the first or last second; the rest of the interval is ignored) that will be scored for the presence or absence of thumb sucking. As noted earlier, using 30-second intervals with MTS will typically permit the observer to detect real changes in thumb sucking during 10-minute to 60-minute observation sessions (Rapp et al., 2008; Devine et al., 2011). Upon completion of each observation session, the observer should calculate the percentage of scored intervals by dividing the number of scored intervals by the total number of intervals in the observation session. In order to evaluate the effects of an intervention on thumb or finger sucking, the results for each observation session should be represented in a linear graph. Figure 13.1 shows hypothetical data collected with 30-second MTS across five observation periods wherein no intervention is implemented for thumb sucking.
Fig. 13.1. Example of hypothetical data collected with 30-second MTS across five observation periods and plotted in a line graph.
Because thumb sucking often occurs only when the child is alone, it may be necessary to observe the behavior surreptitiously while the child is alone (e.g., via video, through an observation window, or during unannounced checks; Friman, Barone, & Christophersen, 1986; Long et al., 1999b; Rapp et al., 1999). For example, Rapp et al. (1999) placed a video camera in the family room of the child’s home to record thumb sucking because the parents reported that the child typically sucked his thumb while watching television there. Videotaped observations can be scored using either CDR or MTS methods, although CDR is preferred as the more rigorous method.
Functional Assessment of Thumb Sucking
Various forms of social reinforcement from the parent often are found to maintain child problem behaviors (e.g., positive reinforcement involving attention from parents, negative reinforcement involving escape from aversive tasks) and thus, treatment involves modifying parental responses to the behavior. However, thumb sucking is a behavior that typically is not maintained by social consequences but through some reinforcing outcome produced by the behavior itself. The reinforcing outcome of thumb sucking is thought to consist of arousal reduction or modulation (automatic negative reinforcement; Friman, Boyd, & Oksol, 2001) or some form of sensory stimulation such as oral or digital stimulation (automatic positive reinforcement; Ellingson et al., 2000; Stricker et al., 2002). Thus, the reinforcer for thumb sucking typically is not under the parents’ control.
Even though thumb sucking is likely to be automatically reinforced, it is nonetheless important to conduct a functional assessment to identify or rule out any possible social reinforcement for the behavior. A functional assessment, typically conducted through interview or direct observation, identifies the antecedents and consequences associated with the behavior (Lennox & Miltenberger, 1989; O’Neill et al., 1997).
In a functional assessment interview, the therapist asks the parents to identify all of the situations in which thumb sucking occurs (antecedents) and asks the parents how they or other caregivers typically respond to the behavior (consequences). If thumb sucking is automatically reinforced, it occurs most often when the child is alone, or occurs across situations, with no consistent reaction from the parent. In many cases, thumb sucking occurs mainly when the child is alone due to a history of punishment for the behavior (e.g., scolding) when it has occurred in the parents’ presence (Rapp et al., 1999). If thumb sucking is socially reinforced, it will be more likely to occur in the presence of the parents or other persons who provide reinforcing consequences. Possible reinforcing consequences for thumb sucking include attention (e.g., expressions of concern, reprimands, or emotional responses contingent on thumb sucking), the provision of other reinforcers (e.g., receipt of a pacifier, candy, or another item to suck on contingent on thumb sucking), or escape from aversive activities or situations (e.g., being removed from an activity or event contingent on thumb sucking). Although it is possible that thumb sucking can be reinforced by such events, results from most studies suggest that thumb sucking is maintained by nonsocial events (e.g., sensory stimulation).
In addition to conducting a functional assessment through an interview and direct observation of the behavior, in some cases, a functional analysis is conducted to identify the reinforcer maintaining thumb sucking (Rapp et al., 1999; Ellingson et al., 2000; Stricker et al., 2002). In a functional analysis, possible reinforcing consequences are manipulated to demonstrate their influence on the target behavior. For example, Rapp et al. (1999) conducted three experimental conditions to determine whether thumb sucking was maintained by social or automatic reinforcement for two 5-year-old boys. In one condition, the parents provided attention contingent on thumb sucking (to assess positive reinforcement). In another condition, the parent made requests and allowed the child to escape the requests contingent on thumb sucking (to assess negative reinforcement). Finally, thumb sucking was recorded when the child was alone to determine whether the behavior persisted in the absence of social reinforcement (to assess automatic reinforcement). Rapp et al. found that thumb sucking occurred almost exclusively in the alone condition. Other researchers have found similar results in their functional analyses of thumb sucking (Ellingson et al., 2000; Stricker et al., 2002).
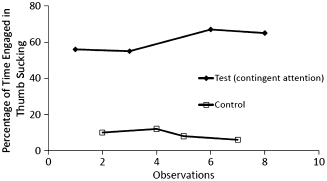
Iwata and Dozier (2008) provided guidelines for conducting multiple forms of brief functional analysis. Given that thumb sucking often is assumed to be automatically reinforced, it can be measured during three to six 10-minute sessions wherein no social interaction is provided to the child. If the behavior occurs at high, stable levels across sessions, the function of the behavior is confirmed and an intervention can be initiated. Figure 13.2 depicts hypothetical data collected with 30-second MTS wherein thumb sucking decreased without social consequences (upper panel) and persisted without social consequences (lower panel). As noted earlier, most studies show that thumb sucking is an automatically reinforced behavior. Nevertheless, if the behavior decreases across the no-interaction sessions, it suggests that thumb sucking is maintained by social consequences, and additional test conditions are needed (Iwata & Dozier, 2008). In a functional analysis test condition, the potential reinforcing consequence is delivered for each instance of the behavior (e.g., attention, escape from a task), and in a control condition, that reinforcer is given freely with no consequence delivered for the behavior. In the event that it is necessary to compare levels of thumb sucking in a test and control condition, practitioners should conduct at least three sessions with each condition to avoid false positives (Kahng & Iwata, 1999; Hanley, Iwata, & McCord, 2003; Bartlett, Rapp, & Henrickson, 2011). Figure 13.3 provides an example of a test versus control functional analysis of thumb sucking. The identified function of thumb sucking then dictates the chosen intervention.
Fig. 13.2. Hypothetical data sets showing thumb sucking extinguishing without social consequence (upper panel) and persisting without social consequences (lower panel).
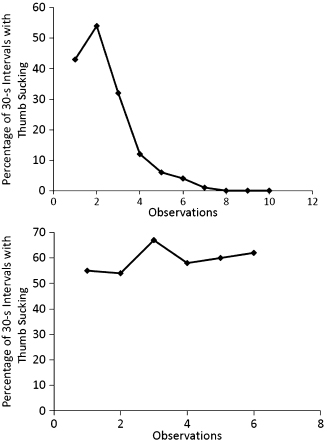
Fig. 13.3. Example of hypothetical results from a brief functional analysis with a test condition (contingent attention) versus a control condition.
Treatment for Thumb Sucking
If the results of a functional assessment or functional analysis identify social reinforcement for thumb sucking, intervention will involve (a) extinction—withholding the reinforcer for thumb sucking, (b) differential reinforcement—providing that reinforcer for the absence of the behavior or for alternative behaviors to replace thumb sucking, and (c) antecedent procedures—providing that reinforcer noncontingently to decrease the motivation for thumb sucking (e.g., Miltenberger, 2012). However, because thumb sucking typically persists in the absence of social reinforcement and often occurs when the child is alone, interventions that alter the antecedents or consequences for the behavior in the absence of the parents or other adults usually are indicated; these procedures are described in the rest of this chapter.
Antecedent Intervention
Antecedent interventions exert their effect on a targeted behavior before that behavior is exhibited. Two types of antecedent interventions for thumb sucking have been evaluated; procedures that involved response prevention and procedures that influence thumb sucking by targeting covarying behaviors.
Response Prevention
A number of apparatuses, such as oral appliances, splints, gloves, and headgear have been used to physically prevent thumb sucking. Although a number of studies have described the use of oral appliances (e.g., Haskell & Mink, 1991; Viazis, 1991; Gawlik, Ott, & Mathieu, 1995; Greenleaf & Mink, 2003) and headgear (e.g., Taylor & Walker, 1997) as interventions for thumb sucking, few, if any, of these studies employed an experimental design to empirically evaluate treatment effects. In contrast, a number of behavioral studies have experimentally demonstrated that finger or thumb splints (e.g., Lassen & Fluent, 1978; Watson & Allen, 1993), gloves (Lewis, Shilton, & Fuqua, 1981; Ellingson et al., 2000), or taped cotton (Rolider & Van Houten, 1988) decreased or eliminated daytime and nocturnal thumb sucking.
In a representative study from this category, Ellingson et al. (2000) first conducted a functional analysis and determined that the finger sucking of two children, aged 7 and 10 years, occurred almost exclusively when each child was alone. In the second phase of the functional analysis, Ellingson et al. found that finger sucking was either greatly reduced or eliminated when adhesive bandages were worn on the fingers, which suggested that finger sucking produced automatic reinforcement in the form of oral or tactile stimulation. Treatment for both participants involved wearing a glove when each was alone (e.g., watching television, lying in bed). For the 10-year-old, the glove immediately eliminated finger sucking. In addition, fading of the glove was accomplished by systematically cutting off pieces over a 5-month period. In contrast, the 7-year-old continued to suck her finger even when she wore multiple gloves. Ultimately, her finger sucking was eliminated using an awareness enhancement device (AED; see later discussion). Although the glove was only effective for one child, parents of both participants rated the glove intervention as highly acceptable.
One limitation in the use of response prevention strategies should be noted. If the child is able to remove the apparatus (glove, splint, etc.) when the parent is not present, its effectiveness will be diminished. Therefore, the parents will need to monitor the child, perhaps surreptitiously, to insure that the apparatus is not removed.
Response Covariation
A number of studies have shown that thumb sucking is eliminated when the sequence or chain of behavioral events that culminates in thumb sucking is interrupted (e.g., Friman, 1988, 1990, 2000; Watson et al., 2002). Similarly, other studies have shown that eliminating thumb sucking, which appears as the first response in a behavioral chain (i.e., one behavior consistently preceded another), also eliminated hair pulling (e.g., Friman & Hove, 1987; Watson & Allen, 1993; Watson, Dittmer, & Ray, 2000) Conversely, Vorndran et al. (2008) found that decreasing hair pulling with behavioral intervention also decreased a child’s untargeted thumb sucking.
Mahalski (1983) reported that as many as 50% of children who display thumb sucking also display attachments to transitional objects such as blankets, pillows, and dolls. In many of these cases, the child obtains one of these objects prior to engaging in thumb sucking. For example, Friman (1988) found that a 5-year-old girl only displayed thumb sucking when she was holding a doll; treatment involved simply withholding access to the doll. Follow-up assessment at 6 months posttreatment showed that thumb-sucking suppression was sustained in the absence of the doll.
Watson et al. (2002) also found that two typically developing brot/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


