Chapter 12 Preimplant Prosthodontics: Overall Evaluation, Specific Criteria, and Pretreatment Prostheses
Implants serve as a foundation for the prosthetic support of missing teeth. However, in the partially edentulous patient, the existing teeth may often require restorations or treatment. The existing conditions of the stomatognathic system should be evaluated and treated, when necessary. As such, preimplant prosthodontic considerations are a vital phase of the overall treatment before implant surgery. For example, the surgical decision to augment or perform osteoplasty before implant surgery is primarily dependent on the desired prosthetic result. Most all conventional forms of construction, from buildings to art form, require a clear vision of the end result before the project is begun.
OVERALL EVALUATION
The preimplant prosthodontic evaluation of the patient’s overall condition closely resembles traditional dentistry. When a restoring dentist first evaluates the prosthetic needs of a patient, an orderly process is required, regardless of the current state of the dentition. In other words, regardless of whether the patient has all teeth or is missing all teeth, after the dentist accepts the responsibility of long-term professional guidance and treatment as necessary, a consistent approach to care is beneficial. There are five initial elements that should be assessed in sequence and treated when indicated. These elements include: maxillary anterior tooth position, the existing occlusal vertical dimension, the mandibular incisor edge position, the maxillary occlusal plane, and the mandibular occlusal plane (Box 12-1). These elements are evaluated in a partially edentulous patient during the initial clinical examination and on mounted diagnostic casts (which may also serve for diagnostic wax-up procedures).
MAXILLARY ANTERIOR TOOTH POSITION
The position of the existing maxillary anterior teeth is first assessed. Most often these natural teeth are adequate in location and incisal edge position. However, if their position is undesirable for any reason, orthodontics or restoration may be indicated. At this point, the evaluation is not for the cosmetic aspects of tooth color or shape, but tooth position is scrutinized. If the maxillary incisor edge is modified in either the horizontal or vertical plane, all other four elements of the stomatognathic system may also need to be changed.
The labial position of the maxillary anterior teeth is first determined with the lip in repose. This is primarily evaluated by overall support of the maxillary lip and its relationship to the balance of the face, especially in relation to the nose and presence or absence of a philtrum in the midline (Figure 12-1).1–7 When the teeth are positioned more labial, the vertical position of the lip is elevated. Likewise, a more palatal position of the maxillary anterior teeth results in a more inferior or extended position of the lip. If the labial or horizontal position is going to be altered, orthodontic therapy is the treatment of choice. On occasion, a prosthetic or surgical approach may be indicated with or without orthodontic treatment.
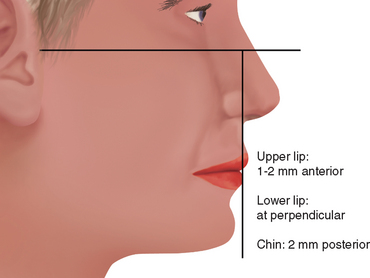
The next step in the evaluation process (when the labial position is acceptable) is the vertical position of the maxillary anterior teeth related to the lip in repose. The maxillary canine is the key for this position. Misch has suggested the canine tip be located approximately 1 mm level with the lip in repose, regardless of the age or sex of the patient (Figure 12-2).8 A horizontal line drawn from one canine tip to the other should be level to the horizon. The central incisors are 1 to 2 mm longer in a horizontal plane to the canines.

EXISTING OCCLUSAL VERTICAL DIMENSION
In order to determine the crown height space (CHS), the overall issue of OVD must be addressed. The patient’s existing OVD should be evaluated early in an implant prosthetic treatment plan, because any modification will significantly modify the overall treatment. Not only will a change in OVD require at least one full arch to be reconstructed, it will also affect the CHS and therefore the potential number, size, position, and angulation requirements of the implants. The OVD is defined as the distance between two points (one in the maxilla and the other directly below in the mandible) when the occluding members are in contact.9 This dimension requires clinical evaluation of the patient and cannot be evaluated solely on the diagnostic casts.
The determination of the OVD is not a precise process, because a range of dimensions is possible without clinical symptoms.10–23 At one time, it was believed OVD was very specific and remained stable throughout a patient’s life. However, this position is not necessarily stable when the teeth are present or after the teeth are lost. Long-term studies have shown this is not a constant dimension and often decreases over time without clinical consequence in the dentate or partially or completely edentulous patient. A completely edentulous patient often wears the same denture for more than 10 years, during which time the OVD is reduced 10 mm or more without symptoms or patient awareness.
The most important effect of OVD on tooth (implant) loading may be the effect on the biomechanics of anterior guidance. The more closed the OVD, the farther forward the mandible rotates and the more Class III the chin appears (Figures 12-3 and 12-4). In a Class II, division 2 patient, the more closed the OVD, the steeper the anterior guidance and the greater the vertical overlap of the anterior teeth. Anterior guidance is necessary to maintain incisal guidance during mandibular excursions to decrease the risk of posterior interferences. These conditions will increase the forces to the anterior teeth. Increasing the OVD has the opposite effect. In general, for the dentate patient it may be more precarious to close an OVD than to open it, because the resulting anterior rotation of the mandible will position mandibular incisor teeth facially in a closer relationship to the maxillary teeth in centric occlusion. In completely edentulous patients restored with fixed implant prosthodontics, a change in OVD in either direction affects biomechanics. Opening the OVD and decreasing the incisal guidance with a resulting bilaterally balanced occlusion may increase forces placed on posterior implants during mandibular excursion. Closing the OVD may increase the forces to anterior implants during any excursion. On occasion, a change in the OVD may also affect the sibilant sounds by altering the horizontal position of the mandible.
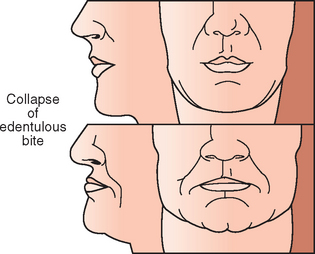

Figure 12-4 The more closed the occlusal vertical dimension, the farther forward the mandibular teeth occlude.
According to Kois and Phillips, three situations primarily mandate the modification of the OVD: (1) esthetics, (2) function, and (3) structural needs of the dentition.12 Esthetics is related to OVD for incisal edge positions, facial measurements, and the occlusal plane. Function is related to the canine positions, incisal guidance, and angle of load to teeth or implants. Structural requirements are related to dimensions of teeth for restoration while maintaining a biological width.
Methods to Evaluate Occlusal Vertical Dimension
The subjective methods to determine OVD include the use of resting interocclusal distance and speech-based techniques using sibilant sounds. Niswonger proposed the use of the interocclusal distance (“freeway space”), which assumes that the patient relaxes the mandible into the same constant physiologic rest position.13 The practitioner then subtracts 3 mm from the measurement to determine the OVD. Two observations conflict with this approach. First, the amount of freeway space is highly variable in the same patient, depending on factors such as head posture, emotional state, presence or absence of teeth, parafunction, and time of recording (greater in the morning). Second, interocclusal distance at rest varies 3 to 10 mm from one patient to another. As a result, the distance to subtract from the freeway space is unknown for a specific patient. Therefore the physiologic rest position should not be the primary method to evaluate OVD. However, it should be evaluated once the OVD is established to ensure a freeway space exists when the mandible is at rest.
Silverman stated that approximately 1 mm should exist between the teeth when making an S sound.14 Pound further developed this concept for the establishment of centric and vertical jaw relationship records for complete dentures.15,16 Although this concept is acceptable, it does not correlate to the original OVD of the patient. Denture patients often wear the same prosthesis for more than 14 years and during this time lose 10 mm or more of their original OVD. Yet all of these patients are able to say “Mississippi” with their existing prosthesis. If speech were related to the original OVD, these patients would not be able to pronounce the S sound because their teeth would be more than 11 mm apart. Therefore the speaking space should not be used as the only method to establish OVD. After the OVD has been determined, the speaking space should be observed, and the teeth should not touch during sibilant sounds. On occasion, a short adjustment period of a few weeks may be required to establish this criterion. Therefore a transitional prosthesis should be used to evaluate this position in case it must be modified before the final restoration.
Kois12 has noted the subjective method of esthetics to establish an OVD is the most difficult to teach inexperienced dental students and therefore is least likely to be initially addressed when teaching the concepts of determining OVD. However, experienced clinicians often value this method more than any other to assess OVD.
After the position of the maxillary incisor edge is determined, the OVD influences esthetics of the face in general. Facial dimensions are directly related to the ideal facial esthetics of an individual and can be easily assessed regardless of the clinician’s experience.17–25 This objective evaluation is usually the method of choice to evaluate the existing OVD or establish a different OVD during prosthetic reconstruction. In addition, it may be performed without the need of additional diagnostic tests.
Facial measurements can be traced back to antiquity, when sculptors and mathematicians followed the golden ratio for body and facial proportions as described by Pythagorus. The golden ratio relates to the length and width of a golden rectangle as 1 to 0.618. Many human body proportions follow the golden ratio because it is considered the most esthetically appealing to the human eye.18–20,25 Leonardo da Vinci later contributed several observations and drawings on facial proportions, which he called divine proportions.21 He observed the distance between the chin and the bottom of the nose (i.e., OVD) was a similar dimension as (1) the hairline to the eyebrows, (2) the height of the ear, and (3) the eyebrows to the bottom of the nose—and each of these dimensions equaled one third of the face.
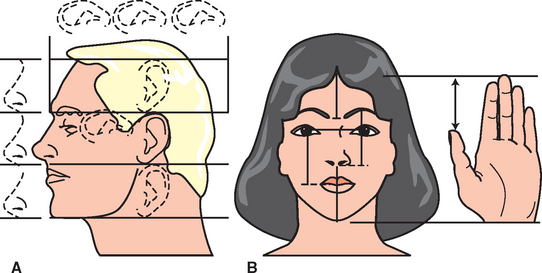
All these measurements do not correspond exactly to each other, but usually do not vary by more than a few millimeters (with the exception of the vertical height of the ear) when facial features appear in balance. An average of several of these measurements may be used to assess the existing OVD. In a clinical study by Misch, the OVD was often slightly larger than the facial measurements listed (more in men than women), but was rarely a smaller dimension.22 The subjective criteria of pleasing esthetics may then be considered after the facial dimensions are within balance to each other.
Radiographic methods to determine an objective OVD are also documented in the literature. Tracings on a cephalometric radiograph is suggested when gross jaw excess or deficiency is noted. Such conditions may stem from vertical maxillary excess, vertical maxillary deficiency, vertical mandibular excess (long chin), vertical mandibular deficiency (short chin), apertognathia or Class II, division 2 (deep bite) situations. Orthodontic treatment planning of a dentate patient often includes a lateral cephalogram and may be used to evaluate OVD (glabella-subnasale, subnasale-menton). The same measurements may be performed on the edentulous patient.26,27
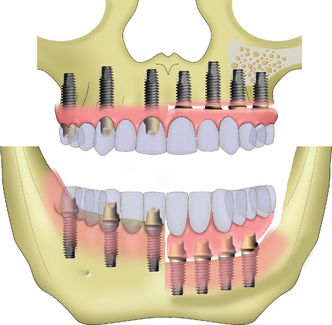
The evaluation of the pretreatment OVD is also very important for the patient wearing a complete maxillary denture opposing a partially edentulous mandible, especially in the case of edentulous posterior segments that are not compensated by a removable partial denture (Kennedy-Applegate Class I). Under these conditions, a combination (Kelly) syndrome may be present and is especially noteworthy if the OVD is within normal limits.28 The clinical symptoms include: (1) maxillary incisor denture position up and rotated back from ideal, (2) lower natural anterior teeth overerupted and beyond the mandibular occlusal plane, (3) horizontal occlusal plane tilted apically in the anterior and occlusally in the posterior regions, (4) enlarged tuberosities encroaching on the mandibular interarch space, (5) maxillary palatal hyperplasia, and (6) highly mobile tissue in the premaxilla. In addition, because the mandibular posterior teeth have been missing many years to develop this syndrome, there is a lack of posterior bone in the mandible to place endosteal implants (Figure 12-6).

The proper maxillary incisal edge position and OVD are especially critical for these patients, because of the incidence of mandibular incisor extrusion beyond the maxillary occlusal plane. The extrusion is usually accompanied by the alveolar process. To position the maxillary incisors properly, the mandibular anterior teeth must be repositioned at the proper incisal plane. Endodontic therapy and crown lengthening procedures usually precede the restorations on the lower arch to obtain a retentive and esthetic restoration.
MANDIBULAR INCISOR EDGE POSITION
After the maxillary incisal edge and the OVD are deemed clinically acceptable, the position of the lower anterior teeth is evaluated. When natural teeth are present, or when a fixed prosthesis is planned in the anterior region, the mandibular teeth incisal edge should contact the lingual aspect of the maxillary anterior natural teeth at the desired OVD position. A vertical overlap with the maxillary anterior teeth is usually in the range of 3 to 5 mm. The incisal guidance is defined as the influence of contacting surfaces of the mandibular and maxillary anterior teeth on mandibular movements.9 The incisal guide angle is formed by the intersection of the plane of occlusion and a line within the sagittal plane determined by the incisal edge of the maxillary and mandibular central incisors when in maximal intercuspation. It is responsible for the amount of posterior tooth separation during mandibular excursions and to do so, it should be steeper than the condylar disc assembly (Christensen’s phenomenon). Therefore any planned prosthesis and associated compensating curves should be developed within these confines. If not, the maxillomandibular arch position may be improper (i.e., in the skeletal Class II patient) and the posterior teeth may exhibit lateral contacts during mandibular excursions. Under these conditions, the masseter and temporalis muscles do not reduce their contraction force during these movements (as they do when only anterior teeth occlude in excursions), and the strong muscles of mastication continue to contract and place an increased force on the entire stomatognathic system.
EXISTING OCCLUSAL PLANES (POSTERIOR MAXILLARY AND MANDIBULAR PLANES OF OCCLUSION)
After the maxillary anterior teeth position, OVD, and mandibular anterior teeth position are deemed acceptable, the horizontal occlusal planes are evaluated in the posterior regions of the mouth. Their position related to the curves of Wilson (mediolateral) and Spee (anteroposterior) and to each other should allow harmonious occlusion with maximum occlusal interdigitation and canine or mutually protected occlusion. Ideally, the maxillary posterior occlusal plane should be parallel to the Camper’s plane (i.e., to the mid-tragus position) (Figure 12-7). The occlusal plane of existing teeth is especially evaluated in partially edentulous patients in relationship to the final implant prosthesis. Odontoplasty, endodontic therapy, or crowns are indicated to remedy tipping or extrusions of adjacent or opposing natural teeth. A pretreatment diagnostic wax-up is strongly suggested to evaluate the needed changes before implant placement. A proper curve of Spee and curve of Wilson are also indicated for proper esthetics and are reproduced in the compensating curves for complete denture fabrication (Figure 12-8).
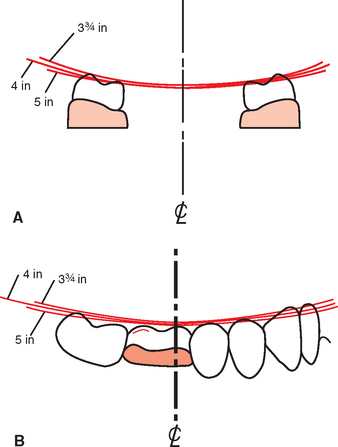
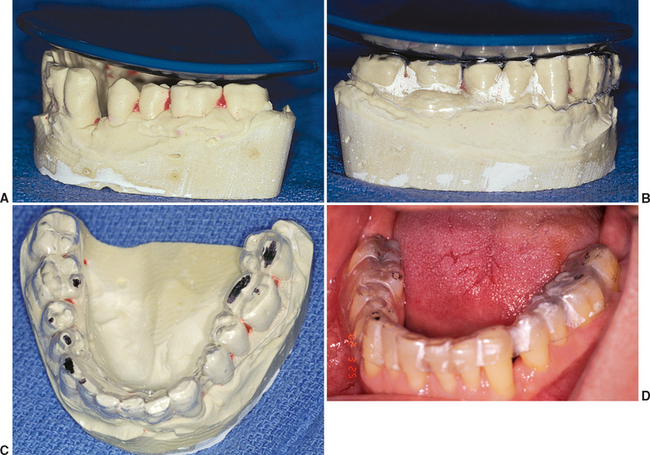
The occlusal plane seems like an obvious step in the patient dental evaluation. However, an evaluation of three-unit fixed prostheses in several large dental laboratories revealed most restoring dentists prepare crowns or three-unit fixed prostheses without correcting the opposing occlusal plane. Apparently, the existing occlusal plane is not routinely evaluated before the fabrication of the prosthesis, or the patient and doctor have decided to compromise the final result and restore the missing teeth to the preexisting poor position. Instead, the restoring dentist should highlight to the patient the extrusion or exfoliation of the surrounding teeth, which is often obvious on a panoramic radiograph or diagnostic casts, after it is noted. The need to restore the missing tooth sooner rather than later is apparent to the patient, because the teeth are already shifting as a result of the arch collapse. If the patient cannot afford the complete treatment plan related to the missing teeth, the opposing arch with the poor occlusal plane should be treated first, not the arch with the missing tooth. In this way, opposing quadrants will ultimately be restored to a proper relationship. Of course, the missing tooth should be replaced before the occlusal plane is compromised again. An occlusal plane analyzer may be used on diagnostic casts to evaluate pretreatment conditions and assist in intraoral occlusal plane correction. Occlusal analyzers are fabricated in several sizes. The average size corresponds to a 4-inch sphere and provides a starting point for ideal curves of Wilson and Spee. Any discrepancy observed on the cast may be corrected in the mouth. A laboratory-assisted template may be fabricated with this intent. In the laboratory, a vacuum or press fit of an acrylic shell is prepared over the cast. The occlusal plane analyzer is then used to evaluate and correct an improper occlusal plane. A hand piece is used to grind the acrylic shell and protruding occlusal cusps on the duplicate diagnostic cast. The clear acrylic shell is then taken intraorally and inserted over the teeth. Any cusp extending through the acrylic shell is recontoured to the level of the surrounding acrylic. As such, the occlusal plane is rapidly corrected to an ideal condition (Figure 12-9).
The CHS in the edentulous site may be significantly reduced as a result of posterior extrusion or exfoliation. The implant drills and implant body insertion often require a posterior crown height space of more than 8 mm from the ideal plane of occlusion, so the hand piece, drill, or implant may be inserted at the correct position and angulation.
SPECIFIC CRITERIA
After the five elements of the existing teeth (restorations) have been evaluated and modified where necessary, several other conditions may modify and hinder the course of implant treatment if overlooked (see Box 12-1 and Appendix A). These conditions should be considered before the final treatment plan is presented to the patient and include the following:
LIP LINES
Lip in Repose
Lip positions are evaluated, including resting lip line, maxillary high lip line (smile), and mandibular low lip line (speech) in relation to the vertical position of the teeth. The lip line positions are especially noted if anterior teeth are to be replaced. The resting lip positions are highly variable, but in general are related to the patient’s age. Older patients show less maxillary teeth at rest and during smiling, but demonstrate more mandibular teeth during sibilant sounds.4 Prosthetic guidelines for incisal edge position established relative to esthetics, phonetics, and occlusion are applied.1–8,29–35
The position of the maxillary incisor in relation to the maxillary lip and the age of the patient is much more variable than the position of the canine. The lip bow in the center of the upper lip rises several millimeters on some females and is barely obvious on others. The higher the lip bow, the more central incisor surface is seen on the patient, regardless of age. Men rarely exhibit an exaggerated lip bow and therefore have a more consistent incisor edge to lip position. The canine position at the corner of the lip is not affected by the lip bow effect. As such, it is a more consistent position and usually corresponds to the length of the resting lip position from 30 to 60 years of age in both males and females.8
High Lip Line
The maxillary high lip line is determined while the patient displays a natural, broad smile.36,37 There are three categories of maxillary lip lines: low, average (ideal), and high (“gummy”). The low lip line displays no interdental papilla or gingiva above the teeth during smiling. The high lip demonstrates all of the interdental papilla and more than 2 mm of tissue above the cervices of the teeth. The clinical characteristics of the average or ideal esthetic smile include a full length of crown exposure (crowns of normal height), a normal tooth position and alignment (lateral incisors may not be completely straight), a normal tooth form, the interdental papilla, and minimal gingival exposure over the cervicals of the teeth (lip at the free gingival margin of the centrals and canines) (Figure 12-10). Approximately 70% of the adult population has a smile line within a few millimeters of the free gingival margin. The FP-1 prosthesis in implant dentistry attempts to reproduce a normal crown contour. However, with a high lip position during smiling, this goal must also include the soft tissue drape around the crown. As a consequence, the aesthetic requirements are much more demanding and often mandate additional surgical steps to enhance the soft and hard tissues before the crown restoration. The selection of an FP-2 and an FP-3 fixed prosthesis is often based solely on the evaluation of the high lip line. An FP-2 prosthesis is easier to fabricate, because it requires fewer porcelain bake cycles.

Approximately 15 to 20% of adults have a low lip line and do not show the interdental papilla when smiling (more males than females) (Figure 12-11). In these patients, the soft tissue drape does not require a primary focus and can often be compromised with a FP-2 restoration, when the patient is notified before treatment. However, an average to high lip position during smiling contraindicates this restoration type because of poor cervical esthetics. The pink porcelain restoration (FP-3) to replace the soft tissue may be esthetic, but is rarely the treatment of choice for single- tooth replacement. On the other hand, in multiple missing adjacent anterior teeth, the pink porcelain is often the treatment of choice, because the soft tissue drape is usually unable to be ideal, even with bone and tissue grafts.

A gummy or high smile line occurs in 14% of the young female patients and 7% of young male patients (Figure 12-12).36 The normal clinical crown width/height ratio is 0.86 for the central incisor, 0.76 to 0.79 for the lateral incisor, and 0.77 to 0.81 for the canine. If the patient demonstrates a band of gingiva over the cervical areas of the teeth, the height of the clinical crowns are evaluated, relative to their width. Esthetic crown lengthening is often a good option when the height of the central clinical crown is less than 10 mm (and the width is greater than 8 mm). Often the effect of crown lengthening is a dramatic improvement and may be accomplished at the same time as the implant surgery.

In patients with a high lip line who are missing all their anterior teeth, the prosthetic teeth can be made longer (up to 12 mm) instead of the average 10 mm height to reduce the gingival display and result in a more esthetic restoration. Therefore the height of the maxillary anterior teeth is determined by first establishing the incisal edge by the lip in repose. Second, the high smile line determines the height of the tooth (from 9 to 12 mm). Third, the width of the anterior teeth is determined by the height/width ratios.
Mandibular Lip Line
The mandibular low lip position is often neglected, with disastrous esthetic results. The mandibular incisors are more visible in middle age and older patients during speaking than maxillary teeth. In addition, lower central incisors are often visible in their incisal two thirds during exaggerated smiles.37,38 Although the maxillary high lip line is evaluated during smiling, the mandibular low lip position should be assessed during speech. In pronunciation of the S sound, or sibilants, some patients may expose the entire anterior mandibular teeth and gingival contour. Patients are often unaware of this preexisting lip position and blame the final restoration for the display of the mandibular gingiva, or complain that the teeth look too long. Therefore it is recommended to make the patient aware of these existing lip lines before treatment and emphasize that these lip positions will be similar after treatment. An FP-3 mandibular restoration may be indicated to restore the patient with a low mandibular lip position.
MAXILLOMANDIBULAR ARCH RELATIONSHIP
Arch relationships are often affected in edentulous ridges. The anterior and posterior edentulous maxilla resorbs toward the palate after tooth loss.39 The width of the alveolar ridge decreases 40% within a few years, primarily at the expense of the labial plate. Consequently, implants are often placed lingual to the original incisal tooth position. The final restoration is then overcontoured facially to restore the incisal two thirds in the ideal tooth position for esthetics. This results in a cantilevered force on the implant body. The maxilla is affected more often than the mandible, because the incisal edge position in the esthetic zones cannot be modified and is dictated by esthetics, speech, lip position, and occlusion. Anterior cantilevered crowns from maxillary anterior implants often require additional implants splinted together and an increase in the anteroposterior distance between the most distal to most anterior implant positions to compensate for the increased lateral loads and moment forces, especially during mandibular excursions.
An anterior cantilever on implants in the mandibular arch may correct an Angle’s skeletal Class II jaw relationship. The maxillary anterior teeth support the lower lip at rest in both Angle’s skeletal Class I and Class II relationships. A traditional complete mandibular denture cannot extend beyond the anatomical support or neutral zone of the lips without decreasing stability of the prosthesis. However, with implants, the denture teeth may be set in a more ideal esthetic and functional position. The anterior cantilever in the mandible is also dependent upon adequate implant number and anteroposterior (A-P) distance between the splinted implants. To counteract the anterior cantilever effect, the treatment plan should provide increased implant support by increasing the surface area by number, size, design, or A-P implant position. In these cases, an RP-4, designed to prevent food impaction, may facilitate daily care and help control the occlusal forces compared with an FP-3 prosthesis.
EXISTING OCCLUSION
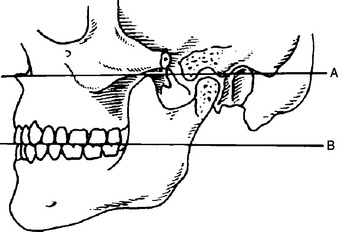
Maximal intercuspation (MI) is defined as the complete intercuspation of the opposing teeth independent of condylar position, sometimes described as the best fit of teeth regardless of the condylar position.9 Centric occlusion is defined as the occlusion of opposing teeth when the mandible is in centric relation (CR).9 This may or may not coincide with the tooth position of maximal intercuspation. Its relationship to CR—a neuromuscular position independent of tooth contact with the condyles in an anterior, superior position—is noteworthy to the restoring dentist because of the potential need for occlusal adjustments to eliminate deflective tooth contacts and the evaluation of their potential noxious effects on the existing dentition and for the planned restoration. Correction of the problems before treatment presents many advantages and may follow a variety of approaches depending on the severity of the incorrect tooth position: selective odontoplasty (a subtractive technique), restoration with a crown (with or without endodontic therapy), or extraction of the offending tooth. The existing occlusion is best evaluated with facebow mounted diagnostic casts and open-mouth bite registration in CR.
Controversy exists as to the necessity to have MI harmonious with CR occlusion. A vast majority of patients around the world do not have such a relationship, yet they do not exhibit clinical pathology or accelerated tooth loss. Therefore it is difficult to state these two positions must be similar. What is important is to evaluate the existing occlusion and the mandibular excursions to consciously decide whether the existing situation should be modified or be maintained. In other words, dentists should determine whether they are going to ignore or control the occlusion of the patient (Figure 12-13).

As a general rule, the more teeth replaced or restored, the more likely the patient is restored to CR occlusion. For example, if a completely edentulous mandible is to be restored with an implant-supported fixed prosthesis, the CR occlusion position provides consistency and reproducibility between the articulator and the intraoral condition and slight changes in OVD to position anterior implant abutments in a more favorable restoration position may be studied and implemented on the articulator without the need to record the new occlusal vertical position on the patient.
CROWN HEIGHT SPACE
The interarch distance is defined as the vertical distance between the maxillary and mandibular dentate or edentate arches under specific conditions (e.g., the mandible is at rest or in occlusion).9 A dimension of only one arch does not have a defined term in prosthetics; therefore Misch proposed the term crown height space (CHS).40 The CHS for implant dentistry is measured from the crest of the bone to the plane of occlusion in the posterior region and the incisal edge of the arch in question in the anterior region (Figure 12-14). The ideal CHS for an FP-1 fixed implant prosthesis should range between 8 and 12 mm. This space accounts for the biological width, abutment height for cement retention or prosthesis screw fixation, occlusal material strength, esthetics, and hygiene considerations around the abutment crowns. Removable prostheses often require more than 12 mm of CHS for denture teeth and acrylic resin base strength, attachments, bars, and oral hygiene considerations.41,42
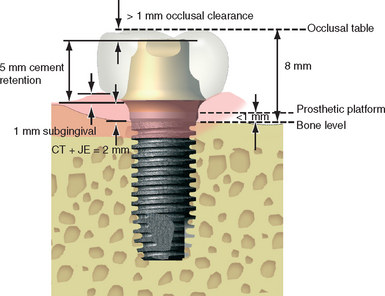
Figure 12-14 The crown height space (CHS) is measured from the occlusal plane to the level of the bone.
Biomechanic Consequences of Excessive Crown Height Space
Mechanical complication rates for implant prostheses are often the highest of all complications reported in the literature43,44 and are often caused by excessive stress applied to the implant-prosthetic system. Implant body or component failure may occur from overload and result in prosthesis failure and bone loss around the failed implants.43 Crestal bone loss may also be related to excessive forces and often occurs prior to implant body fracture.
The biomechanics of CHS are related to lever mechanics. The issues of cantilevers and implants were demonstrated in the edentulous mandible where the length of the posterior cantilever directly related to complications or failure of the prosthesis.44 Rather than being a posterior cantilever, the CHS is a vertical cantilever and therefore is also a force magnifier.
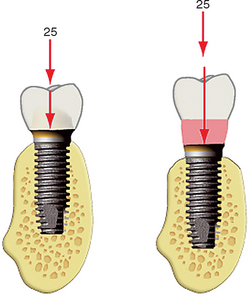
When the direction of a force is in the long axis of the implant, the stresses to the bone are not magnified in relation to the CHS (Figure 12-15). However, when the forces to the implant are on a cantilever or a lateral force is applied to the crown, the forces are magnified in direct relationship to the crown height. As discussed in Chapter 6, Bidez and Misch evaluated the effect of a cantilever on an implant and its relation to crown height.45,46 When the crown height is increased from 10 to 20 mm, two of six of these moments are increased 200%. When the available bone height is decreased, the CHS is increased.
An angled load to a crown also magnifies the force to the implant. A 12-degree force to the implant increases the force by 20%. This increase in force is further magnified by the crown height. For example, a 12-degree angle with a 100-N force will result in a force of 315 N-mm on a crown height of 15 mm.46 Maxillary anterior teeth are usually at an angle of 12 degrees or more to the occlusal planes. Therefore even implants placed in an ideal position are usually loaded at an angle. In addition, maxillary anterior crowns are often longer than any other teeth in the arch, so the effects of crown height cause greater risk. The angled force to the implant may also occur during protrusive or lateral excursions, because the incisal guide angle may be 20 degrees or more. Anterior implant crowns will therefore be loaded at a considerable angle during excursions compared with the long axis of the implant. As a result, an increase in the force to maxillary anterior implants should be compensated for in the treatment plan.
Most forces applied to the osteointegrated implant body are concentrated in the crestal 7- to 9-mm bone, regardless of implant design and bone density. Therefore implant body height is not an effective method to counter the effect of crown height. Moderate bone loss before implant placement may result in a crown height—bone height ratio greater than 1, with greater lateral forces applied to the crestal bone than in abundant bone (in which the crown height is less). A linear relationship exists between the applied load and internal stresses.47,48 Therefore the greater the load applied, the greater the tensile and compressive stresses transmitted at the bone interface and to the prosthetic components. The greater the CHS, the greater number of implants usually required for the prosthesis, especially in the presence of other force factors. This is a complete paradigm shift to the concepts advocated originally with many implants in greater available bone and small crown heights and fewer implants with greater crown heights in atrophied bone (Figure 12-16).
Because an increase in the biomechanical forces are in direct relationship to the increase in CHS, the treatment plan of the implant restoration should consider stress-reducing options whenever the CHS is increased. Methods to decrease stress are presented in Box 12-2.40,41
Excessive Crown Height Space
Crown height space is excessive when greater than 15 mm. Treatment of excessive CHS as a result of vertical resorption of bone before implant placement includes surgical methods to increase bone height or stress reduction methods to the prosthesis. Several surgical techniques may be considered to increase bone height, including block onlay bone grafts, particulate bone grafts with titanium mesh or barrier membranes, interpositional bone grafts, and distraction osteogenesis.41,42,49
In the case of removable prostheses with mobility and soft tissue support, two prosthetic levers of height should be considered. The first is the height of the attachment system to the crest of the bone. The greater the height distance, the greater the forces applied to the bar, screws, and implants. The second CHS to consider is the distance from the attachment to the occlusal plane. This distance represents the increase in prosthetic forces applied to the attachment. Therefore in a CHS of 15 mm, an O-ring may be 7 mm from the crest of bone, resulting in a lever action of 7 mm applied to the implants. The distance from the rotation point of the O-ring to the occlusal plane may be an additional 8 mm. Under these conditions, a greater lever action is applied to the prosthesis than to the implant interface. This results in increased instability of the restoration under lateral forces.42
A CHS greater than 15 mm means a large amount of metal must be used in the substructure of a traditional fixed restoration to keep porcelain to its ideal 2-mm thickness (Figure 12-17). Control of surface porosities of metal substructures after casting becomes increasingly difficult, because their different parts cool at different rates.50 If not controlled properly, both of these factors increase the risk of porcelain fracture after loading.51 For excessive CHS, considerable weight of the prosthesis (approaching 3 oz of alloy) may affect maxillary trial placement appointments, because the restoration does not remain in place without the use of adhesive. Because noble metals must be used to control alloy’s heat expansion or corrosion, the cost of such implant restorations is dramatically increased. Proposed methods to produce hollow frames to alleviate these problems include using special custom trays to achieve a passive fit, which can double or triple the labor costs.52

An alternative method to fabricate fixed prostheses in situations of CHS 15 mm or greater is the fixed complete denture or hybrid prosthesis, which has a smaller metal framework, denture teeth, and acrylic resin to join these elements together (Figure 12-18). This type of fixed prosthesis is often indicated for implant restorations with a large CHS. On occasion, undercontoured interproximal areas are designed by the laboratory in restorations of large CHS space to assist oral hygiene, and have been referred to as high-water restorations. This is an excellent method in the mandible; however, it results in food entrapment, affects air flow patterns, and may contribute to speech problems in the anterior maxilla.

Reduced Crown Height Space
Issues related to CHS are accentuated by an excessive CHS that places more forces on the implant and prosthetic system, and reduced CHS makes the prosthetic components weaker. A reduced CHS has biomechanical issues related to a reduced strength of implant material or prosthetic components, an increased flexibility of the material, and a reduction of retention requirement of the restoration. The fatigue strength and flexure of a material is related to its radius to the power of 4. In fixed restorations, the flexure of the reduced-diameter material may cause porcelain fracture, screw loosening, or uncemented restorations. Therefore in the situation of reduced CHS, material failures are more likely (Box 12-3).
Box 12-3 Reduced Crown Height Space
When the opposing teeth are in the correct position and the CHS is insufficient, additional space may be gained surgically with osteoplasty and soft tissue reduction of one arch, provided adequate bone height remains after the procedure for predictable implant placement and prosthetic support (Figure 12-19). If a removable implant-supported prosthesis is planned, an aggressive alveoloplasty should often be performed after tooth extraction to provide adequate prosthetic space.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


