Metal Ceramic Framework Design
Robert P. Berger
Introduction
This chapter is about connecting the gap between dental technology and patient health. There exists a special relationship between dental technology and good health, and among dental laboratory technicians, dentists, and patients. When a patient has a problem, the dentist must diagnose the cause of the problem and prescribe a remedy. The prescription is then given to the laboratory technician, who accepts the responsibility for fabricating the prescribed prosthesis so that it fulfills the patient’s needs and solves or aids in the solution of the patient’s problem. If either the dentist or the technician misses a beat, it is the patient who will suffer. It is a special relationship in which the health and well-being of the patient is a function of both the dentist and the technician and their combined abilities to diagnose, prescribe, and fabricate the correct remedy to the problem. Framework design, esthetics, and physiology are all partners in the patient’s health.
Proper design of the metal ceramic framework controls the morphology of the restoration. It also promotes good oral health.
Esthetics and strength are the primary reasons why a metal ceramic restoration would be prescribed. Otherwise, technologists under the direction of the dentist would just make all-metal restorations. Fortunately, that is not what our culture is all about. Our culture has developed the desire to look natural, not reconstructed.
A metal ceramic restoration uses the best advantages of both materials, the strength of the metal, and the beauty of a veneer that defies the human eye to differentiate it from the real thing. When metal ceramic restorations are correctly constructed, the patient realizes significant benefits, not only in terms of esthetics but also in terms of oral health. Good physiology is good esthetics.
The benefits of a properly designed metal ceramic framework are as follows: (1) improved appearance, (2) absence of oral pain, (3) better oral hygiene, (4) total overall bodily health, and (5) a feeling of self-confidence and self-worth. When it has been decided that a metal ceramic prosthesis is the restoration of choice, it must be assured that it is made in such a way that the maximum benefits of good oral physiology and natural esthetics are achieved. Is that possible? Yes, esthetics and physiology are partners in good health.
There are three areas of framework design that promote proper construction of fixed prostheses and will ensure good oral health of the hard and soft tissues: marginal fit, contour control, and lingual metal band design. These are the factors that determine structural integrity, esthetic appearance, and the physiologic response to the fixed partial denture or individual crown.
The accuracy of the marginal fit has a significant influence on maintaining the health of the hard and soft tissues. There are three types of inaccuracies pertaining to marginal fit: short margin, overexpansion, and underexpansion. A well-fitting crown placed on an abutment protects the dentinal hard tissues by sealing the prepared tooth from the bacterial environment of the oral cavity. The short margin, whether caused by a discrepancy between the preparation and the impression or an error in the fabrication of the restoration, is an open invitation to plaque attachment leading to inflammation.
Overexpansion
Overexpansion can cause the cast restoration to rock on the prepared tooth, opening either the facial or lingual margin, but, even more detrimental, if seated, the overexpanded restoration creates an overhang extending beyond the margin of the tooth. The overhang creates an area for plaque collection. The shelf created by the overexpansion of the casting prevents debris from being easily removed by the patient. The persistence of this condition will lead to a deterioration in the health of the surrounding tissues (Fig 11-1).
Fig 11-1 An overexpanded crown will collect plaque subgingival to the shelf created by the overhang. The plaque cannot be easily removed by the patient, a situation that can lead to inflammation of the surrounding gingival tissue.
Underexpansion
Underexpansion makes fitting of the cast restoration extremely difficult because the internal dimension of the casting is smaller than the preparation. Machining the internal surface of the casting, ie, making its internal dimension larger, may allow the casting to seat fully on the prepared tooth, but it will not eliminate the physiologic negative of a short margin. The marginal periphery of an underexpanded cast crown is always smaller (less in circumference) than the marginal periphery of the prepared tooth.
Placing an underexpanded or overexpanded crown, which has been machined to fit, will always leave an exposed surface around the periphery of the prepared tooth (Fig 11-2).
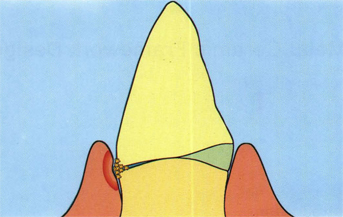
Fig 11-2 An underexpanded or overexpanded crown will always have an open margin because the periphery of the margin of this crown is different than the margin periphery of the prepared tooth.
Control of marginal fit
The accuracy of the fit of a crown casting can be controlled by tooth preparation, complete and accurate impressions, accurate cast pouring, use of controlled thickness cement spacers, fabrication of accurate wax patterns, and the control of investment mold expansion.
Tooth preparation
A shoulder, beveled shoulder with gingival metal band, or chamfer design is preferable. The feather-edge design should not be used except where absolutely unavoidable. Kuwata1 illustrated that the feather-edge margin design causes an overcontour of the ceramic veneer at the gingival margin of a restoration due to insufficient tooth reduction. Shillingburg et al2 demonstrated that the shoulder design, adequately reducing the tooth structure just above the preparation margin, allowed for the thickness of the porcelain veneer. Sufficient reduction at the gingival margin ensures that the gingival contour of the crown will be in line with the emergence profile of the tooth.
Accurate complete impressions
Full-arch impressions will allow the dental technician to construct a prosthesis that will be in balance with the patient’s existing dentition by having the advantage of being able to see a full view of the patient’s oral architecture. Quadrant-arch impressions will not permit the technician to make a bilateral comparison of the patient’s existing morphology and leave occlusal function to guesswork.
Accurate cast pouring
Correct measurement of the gypsum water-to-powder ratio will ensure controlled expansion of the die stone, producing an exact duplication of the patient’s dentition in the dental cast. The dental cast is the first step in the prosthesis fabrication process. Although the produced prosthesis may accurately fit the dental cast, an inaccurate cast will create an inaccurate fit of the prosthesis on the patient’s prepared teeth. A poor physiologic result is inevitable when the prosthesis fits inaccurately.
Spacers
Cement spacer thickness must be controlled to ensure accurate fit of the cast crowns. Far too often the application thickness of the spacer is unknown. Frequently the spacer thickness is insufficient, not allowing the minimum required relief of 25 μm on the die surface.3,4 When the relief is less than required, the crown when cemented will be prevented from fully seating on the patient’s prepared tooth because of the film thickness of the cement that lines the internal surfaces of the crown. This condition will not only necessitate occlusal adjustment but will also leave the crown short of marginal seal, creating an unesthetic appearance at the junction of the crown and the tooth and leading to other physiologic problems associated with poor marginal fit.
Accurate wax patterns
A cast crown will never fit the die any better than the wax pattern that was made to generate the casting fit. Hand application of wax to the die has shown to be an extremely demanding technique. The shrinkage of inlay waxes necessitated the frustrating and sometimes inaccurate procedure of margin resealing. Antiquated inlay waxes, originally designed for making wax patterns directly in the patient’s mouth, belong in the dental office. Today, progressive, highly skilled dental technicians working in modern dental laboratories use a new generation of wax known as Microcrystalline Dipping Wax (Belle de St. Claire, Chatsworth, Calif). This new formulation of wax has proven to be superior for the indirect waxing technique. Because of the low shrinkage property of the microcrystalline wax, the dipped wax coping can also be used to produce the marginal area of the pattern. When only one wax is used to construct the entire area of the pattern that contacts the surface of the die, including the marginal seal, the expansion and contraction of the wax throughout the pattern will be uniform. When expansion of the wax pattern is uniform, hygroscopic expansion of the casting investment will be uniform. Uniform pattern expansion ensures that the internal surfaces of the cast crown will equally fit all surfaces of the die. The strength and malleability of the dipping wax permit handling without distortion, and the high fusing temperature (165°F/melting point) of the new wax resists heat distortion when carving waxes, used to build contour, are added to its surface. The use of the dipped wax coping for the initia/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


