Chapter 10
Treat or Refer?
Aim
This chapter considers how to assess when younger patients should be treated within a general dental practice setting and when they should be referred for specialist care.
Outcome
Having read this chapter the practitioner should understand which cases can be managed safely in general practice and which should be referred for specialist care. The reader will also have gained knowledge about the appropriate information to include in a referral letter for younger periodontal patients.
Making the Decision to Treat or Refer
The decision to treat or refer a young patient will be dependent on three issues (Fig 10-1):
-
the general dental practitioner’s expertise
-
patient-centred factors
-
complexity of the case.
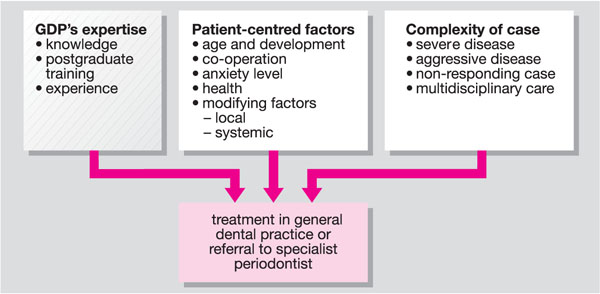
Fig 10-1 Factors influencing the decision to treat or refer.
The British Society of Periodontology has developed a referral policy based on a patient having been screened for periodontal diseases using the Basic Periodontal Examination (BPE). Although primarily targeted at adults, the principles described below can be applied successfully to younger patients. Not every patient with the features listed in Box 10-1 will need specialist care; however, the need for referral should be considered for such patients.
Box 10-1
Younger Patients Who May Need Referral
Diagnosis of aggressive periodontitis
Incipient chronic periodontitis not responding to non-surgical therapy provided by the practice team
Systemic medical conditions associated with periodontal destruction (see Chapters 5, 7 and 8)
Genetic conditions predisposing to periodontal destruction (Chapter 7)
Drug-induced gingival overgrowth (Chapter 5)
At risk from delivery of periodontal care (e.g. risk of infective endocarditis)
Local factors (e.g. root morphology) affecting prognosis
Requiring evaluation for periodontal surgery
Requiring diagnosis of rare and complex clinical pathology (Chapters 6 and 7)
Requiring complex multidisciplinary medical and dental care
Another useful service that is provided by specialist periodontists is the provision of a specialist opinion and treatment plan. This may be valuable in the situation in which the dentist is happy to treat the patient but wants confirmation of a diagnosis or assistance with planning the management. The specialist may suggest a division of the therapy between the practice and a specialist centre. This can be particularly helpful when long distances are involved and the patient/parent find it easier to have most of their care delivered locally.
The Referral Process
The Referral Letter
The principal method of referring a patient to a specialist is still via a written referral letter. It has been shown that the quality of referral letters is considerably better when a referral pro forma is used (Snoad et al. 1999). Having a pro forma or some other form of template can prevent key pieces of information from being omitted as well as making the process of writing the letter simpler. An example referral letter is shown in Fig 10-2 highlighting the key points that should be included, although there may be additional details relevant in individual cases which should be added as appropriate. Copies of probing pocket depth and bleeding charts may be of value if these are available.
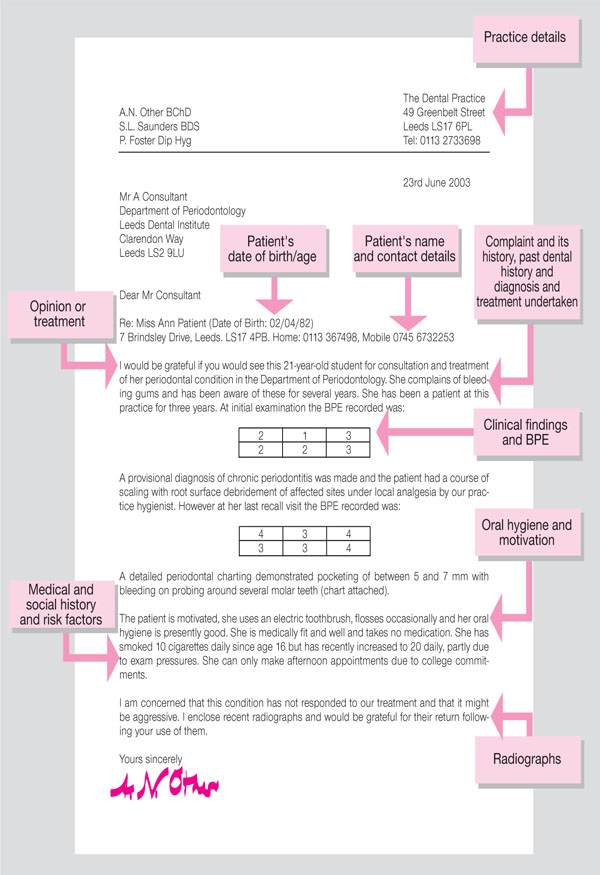
Fig 10-2 Example of a periodontal referral letter for a young patient.
It is important that the radiation dosage from radiographs is kept as low as possible in children as the tissues of younger people are more radiosensitive than those of adults. To minimise the dose and justify the taking of radiographs it is considered best practice to have available previous radiographs and the practitioner should send relevant radiographs with the referral. Many specialists will specifically ask the referring dentist to forward radiographs if none have been sent with the original letter. Previous radiographs may reduce the need for further films at the consultation visit and may help to assess disease progression if films over a number of years are available. Practitioners may be reluctant to send in radiographs for a number of reasons including their potential loss. It is worthwhile including in the referral letter a specific request for return of the radiographs after their use. Many specialists are able to copy radiographs and return the originals to the practitioner.
Periodontal therapy can be divided into three phases (see Chapter 8): initial, cor/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


