10 Reactive Keratotic Lesions (Nonleukoplakias)
White Lesions
White lesions are some of the more commonly biopsied lesions and one of the most challenging for general pathologists and dermatopathologists. This is particularly because of confusion over nomenclature (especially over the term leukoplakia) and difficulty recognizing oral frictional keratoses, the two most common being morsicatio mucosae oris and benign alveolar ridge keratosis. There are also other frictional/reactive keratoses that are not as well defined histologically. Table 10-1 provides a list of mucosal conditions that are usually white; these are discussed subsequently and in other chapters.
TABLE 10-1 Histologic Diagnoses for Papulomacular White Lesions
| Developmental/Hereditary |
The oral mucosa appears white for several reasons:
• Presence of keratin in a normally nonkeratinized site
• Hyperparakeratosis or hyperorthokeratosis in a normally keratinized site
• Coagulation of superficial keratinocytes
• Alteration of the epithelial cells because of abnormal keratin formation or aggregation (see Chapter 2)
• Nonepithelial changes such as underlying scarring and fibrosis
When a mildly irritating substance comes in contact with the mucosa or when there is mild physical surface trauma, superficial cells become edematous and degenerate until the effects of the irritation (contacting chemical or physical irritation) are diluted, beyond which the keratinocytes appear normal. Such changes are seen in leukoedema and morsicatio mucosae oris. Smokeless tobacco lesions in particular show this effect, although over time carcinogens from tobacco may result in significantly keratotic and dysplastic lesions. Aspirin, however, is so caustic that it leads to complete destruction of the epithelial layer, resulting in ulceration and necrosis rather than a keratotic lesion, although the earliest changes may be leukoedema. Irritant contact stomatitis results in a clinical erythematous lesion with spongiosis as its main histologic feature (see Chapter 7). Correlating the histopathologic and clinical findings is key to arriving at an accurate diagnosis.
Reactive Lesions
Leukoedema
Clinical Findings
• Present in up to 90% of the population; more readily discerned in dark-skinned individuals; history of mild surface injury such as smoking, sucking, or use of strong oral rinses or toothpaste
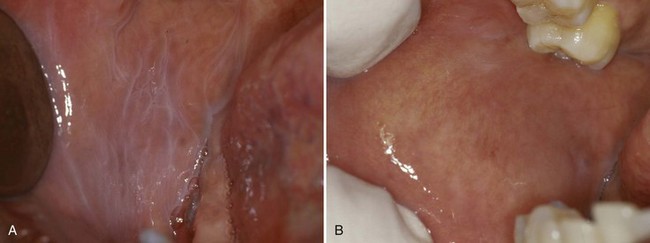
• Delicate lacy, gray-white lines on the buccal mucosa or tongue (nonkeratinized site) that disappear with stretching (Fig. 10-1)
Etiopathogenesis and Histopathologic Features
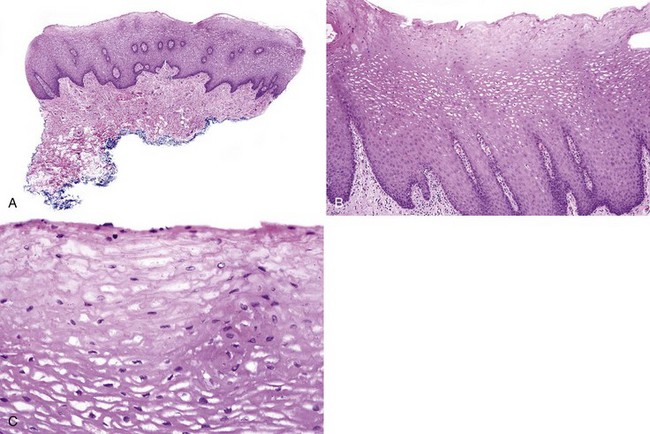
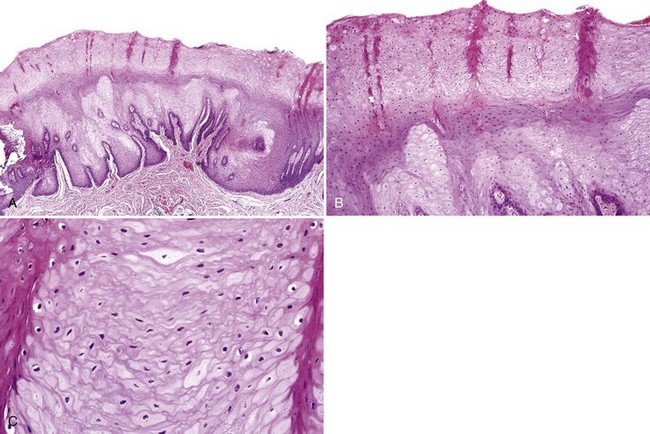
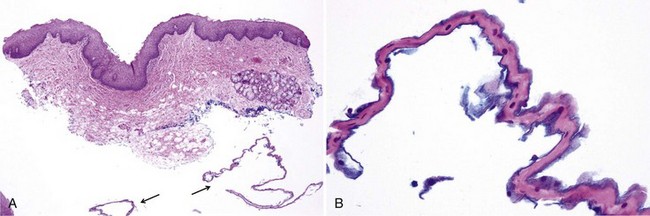
• Keratinocyte edema of superficial cells appear pale and ballooned; absent nuclei may be due to plane of section or degeneration; cell membranes have compacted “jigsaw” puzzle appearance; deeper cells show perinuclear halos (but do not represent koilocytes because they lack other nuclear characteristics); usually, minimal-to-no keratin is noted, although keratin chevrons may be present (Figs. 10-2 and 10-3).
• Benign epithelial hyperplasia with minimal-to-no inflammation may be seen.
Canaan TJ, Meehan SC. Variations of structure and appearance of the oral mucosa. Dent Clin North Am. 2005;49:1-14.
Heyl T, Raubenheimer EJ. Sucking pads (sucking calluses) of the lips in neonates: a manifestation of transient leukoedema. Pediatr Dermatol. 1987;4:123-128.
Versteeg PA, Slot DE, van der Velden U, van der Weijden GA. Effect of cannabis usage on the oral environment: a review. Int J Dent Hyg. 2008;6:315-320.
Contact Desquamation
Clinical Findings
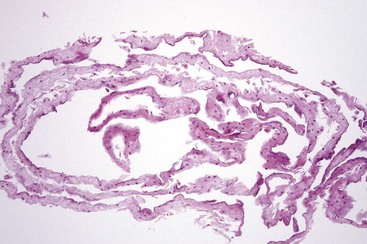
• Painless, thready white fragments lie on the mucosa (usually nonkeratinized sites) that easily peel off, leaving normal mucosa (Fig. 10-4); surrounding leukoedema may be seen; patients may also develop contact cheilitis.

Francalanci S, Sertoli A, Giorgini S, et al. Multicentre study of allergic contact cheilitis from toothpastes. Contact Dermatitis. 2000;43:216-222.
Kowitz G, Jacobson J, Meng Z, Lucatorto F. The effects of tartar-control toothpaste on the oral soft tissues. Oral Surg Oral Med Oral Pathol. 1990;70:529-536.
Kuttan NA, Narayana N, Moghadam BK. Desquamative stomatitis associated with routine use of oral health care products. Gen Dent. 2001;49:596-602.
Frictional/Factitial Keratoses
The majority of hyperparakeratotic and hyperorthokeratotic lesions in the oral cavity are reactive, frictional keratoses. Two histologically well-defined frictional keratoses in the oral cavity are morsicatio mucosae oris (generally on the nonkeratinized mucosa) and benign alveolar ridge keratosis (lesions on the keratinized mucosa). The linea alba on the buccal mucosa is considered a variation of normal but is a severe localized leukoedema or a mild morsicatio mucosae oris (Fig. 10-7, A)

Morsicatio Mucosae Oris (Morsicatio Buccarum, Pathominia Mucosae Oris)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


