Chapter 1
The Periodontal Team
Aim
This chapter aims to provide the general dental practitioner (GDP) with an insight into the development and role of professionals complementary to dentistry within the context of the management of periodontal diseases.
Outcome
As a result of reading this chapter the practitioner should have an understanding of how the periodontal team has evolved and the legally permitted duties of dental hygienists and dental therapists.
Introduction
It is in the primary care setting that the vast majority of periodontal disease is diagnosed and managed. The team involved in patient care may be small, involving only the dentist, dental hygienist and dental nurse. Conversely, the team may work together in a large polyclinic where periodontal care is one of many specialist dental services offered. In such situations the periodontal specialist will be available for the diagnosis and management of the more complex cases.
In its broadest sense, the dental team reaches beyond the high street surgery to include the secondary care services in hospital periodontal departments where the consultant in restorative dentistry and his or her team will offer advice and, where appropriate, treatment of referred cases.
In order to obtain the most appropriate care for an individual patient the GDP will refer the patient to other team members to utilise their skills, knowledge and experience to achieve the desired treatment outcomes. Rather than this referral process being considered as a hierarchical model, it is suggested that it be considered in a circular form with the GDP at the centre. It is the GDP with whom the patient is registered and it is the GDP to whom the patient returns for continuing care (Fig 1-1). The role of the GDP is an infinite one! The other team members have important skills to offer, but their roles are finite ones, clearly defined by the practitioner’s referral request or treatment plan.
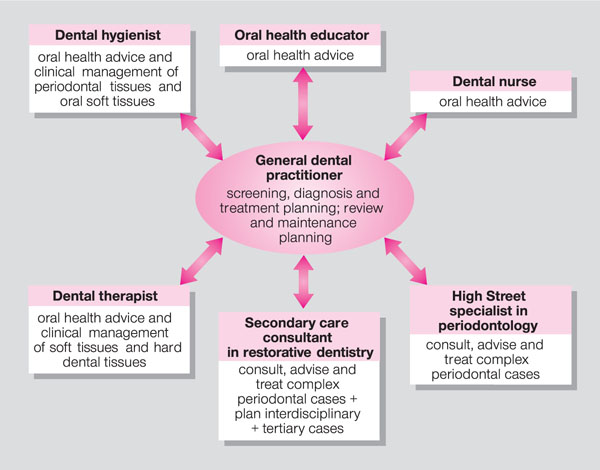
Fig 1-1 Members of the periodontal team.
By co-ordinating the referral process the practitioner plays the key role in consolidating the treatment and ensuring that the patient is informed of the reasons behind the referral. The role of the practitioner as the team leader is explored further in Chapter 3, but by way of introduction to “working together” this chapter will focus on the evolution of the professionals complementary to dentistry and the skills these team members have to offer.
The Dental Hygienist
Although dental hygienists were first trained in the United States in 1913, there was no formal training in the UK until 1943, in the Royal Air Force. During the next 20–30 years schools of dental hygiene were founded and attached to dental schools, but they trained relatively few hygienists compared to dentists. Enrolment with the General Dental Council (GDC) became mandatory in 1957.
The original concepts of patient education and prevention of periodontal diseases remain the linchpin of the dental hygienist’s role, but the range of permitted duties has expanded in recent years in line with the current concepts of team management for patients with oral diseases. Dually qualified dental hygienists/therapists now receive education to diploma and degree levels in universities alongside undergraduate dental students. This enhances the periodontal team concept within the workplace.
The changing patterns of oral disease and the increasing public awareness and demand for oral health was the driver behind the Nuffield Inquiry into Education and Training of Personnel Auxiliary to Dentistry in 1993. This extensive inquiry examined the role of dental auxiliary personnel, and stimulated widespread debate on a number of key issues surrounding the development of the dental team. Following this the GDC set up the Dental Auxiliaries Review Group (DARG), to prepare appropriate recommendations in relation to all classes of dental auxiliary. The committee reported in 1998, setting out proposals on permitted duties, entry requirements and registration. It was also recommended that the team concept for future practice should be promoted through the training of dentists and dental auxiliaries in close association with each other.
Subsequently, in 1999, the GDC announced a new era for professionals complementary to dentistry. The council supported statutory registration of all members of the dental team and the widening of clinical roles after appropriate education and training. Although the term dental hygienist remained protected, as it was a role with which the general public was familiar, the dental hygienist became incorporated into a wider group subsequently named Professionals Complementary to Dentistry (PCD). The GDC emphasised that entry to the register would be on the basis of appropriate education and that each PCD should practise only under the delegated authority of a registered dentist.
It was the expressed intention of the GDC that all PCDs should continue to work within the dental team within which the dentist would remain responsible for diagnosis, treatment planning and the quality control of the treatment provided (Fig 1-2).

Fig 1-2 The team and team leader.
Legally Permitted Duties
Until such time as the GDC is able to register all PCDs, dental hygienists and dental therapists may practise dentistry to the extent of the Dentists Act 1984 and the 1986 Dental Auxiliaries Regulations, with amendments in 1991 and 2002. It is an offence to practise outside these limits.
They are permitted to work “under the direction of a registered dentist”. This implies that the dentist has examined the patient and indicated in writing the course of treatment to be pro/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


