CHAPTER 1 Partially Edentulous Epidemiology, Physiology, and Terminology
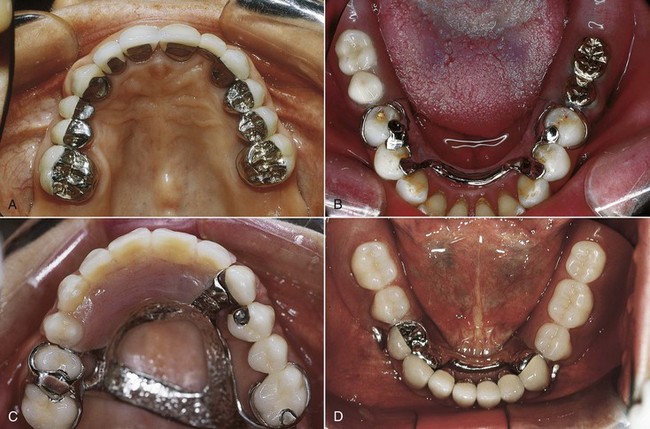
Current practice in the management of partial tooth loss involves consideration of various types of prostheses (Figure 1-1). Each type of prosthesis requires the use of various remaining teeth, implants, and/or tissues, and consequently demands appropriate application of knowledge and critical thinking to ensure the best possible outcome given patient needs and desires. Although more than one prosthesis may serve the needs of a patient, any prosthesis should be provided as part of overall management that meets the basic objectives of prosthodontic treatment, which include (1) the elimination of oral disease to the greatest extent possible; (2) the preservation of the health and relationships of the teeth and the health of oral and paraoral structures, which will enhance the removable partial denture design; and (3) the restoration of oral functions that are comfortable, are esthetically pleasing, and do not interfere with the patient’s speech. It is critically important to emphasize that the preservation of health requires proper maintenance of removable partial dentures. To provide a perspective for understanding the impact of removable partial denture prosthodontics, a review of tooth loss and its sequelae, functional restoration with prostheses, and prosthesis use and outcomes is in order.
Familiarity with accepted prosthodontic terminology related to removable partial dentures is necessary. Figures 1-2 and 1-3 provide prosthesis terms related to mandibular and maxillary frameworks, and Appendix A provides a review of selected prosthodontic terms. Additional terminology can be reviewed in The Glossary of Prosthodontic Terms1 and a glossary of accepted terms in all disciplines of dentistry, such as Mosby’s Dental Dictionary, second edition.2
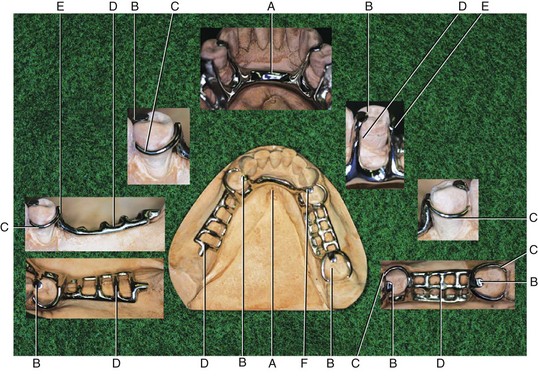
Figure 1-2 Mandibular framework designed for a partially edentulous arch with a Kennedy Classification II, modification 1 (see Chapter 3). Various component parts of the framework are labeled for identification. Subsequent chapters will describe their function, fabrication, and use. A, Major connector. B, Rests. C, Direct retainer. D, Minor connector. E, Guide plane. F, Indirect retainer.
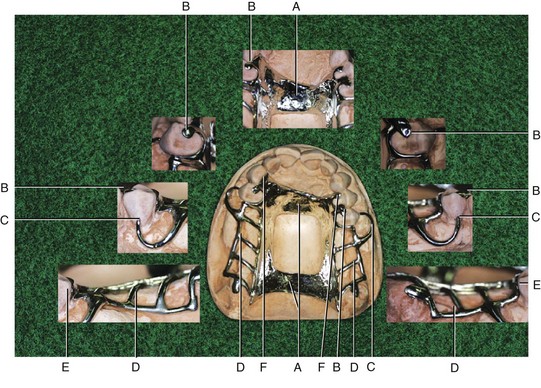
Figure 1-3 Maxillary framework designed for a partially edentulous arch with a Kennedy Classification I (see Chapter 3). As in Figure 1-2, component parts are labeled for identification. A, Major connector. B, Rests. C, Direct retainer. D, Minor connector. E, Guide plane. F, Indirect retainer.
Tooth Loss and Age
It should come as no surprise that tooth loss and age are linked. A specific tooth loss relationship has been documented with increasing age because some teeth are retained longer than others. It has been suggested that in general an interarch difference in tooth loss occurs, with maxillary teeth demonstrating loss before mandibular teeth. An intraarch difference has also been suggested, with posterior teeth lost before anterior teeth. These observations are likely related to respective caries susceptibilities, which have been reported (Table 1-1). Frequently the last remaining teeth in the mouth are the mandibular anterior teeth, especially the mandibular canines, and it is a common finding to see an edentulous maxilla opposing mandibular anterior teeth.
| High Risk | Lower 6 and 7 | Mandibular 1st and 2nd molars |
| Upper 6 and 7 | Maxillary 1st and 2nd molars | |
* If tooth loss parallels caries activity, caries risk may be a proxy for tooth loss.
Data from Klein H, Palmer CE: Studies on Dental Caries: XII. Comparison of the caries susceptibility of th/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


