Introduction
The purpose of this study was to investigate the success rate of midpalatal miniscrews used for orthodontic anchorage and the factors affecting clinical success.
Methods
One hundred twenty-eight consecutive patients (101 female, 27 male; mean age, 23.4 years), who received a total of 210 miniscrews in the midpalatal suture area, were examined. Success rates were determined according to 10 clinical variables.
Results
The overall success rates were 88.20% for the total number of patients and 90.80% for the total number of miniscrews. There were no significant associations among success rate and sex, total period of treatment with miniscrews, diameter of miniscrews, types of tooth movements, and variables that represent sagittal and vertical skeletal relationships (ANB, FMA, and Sn-GoGn). The operator’s learning curve, patient’s age, area (midpalatal or parapalatal), and splinting significantly influenced the success rates. After adjusting for other variables, only 1— splinting—showed a significant effect on the success rate.
Conclusions
The joining of 2 miniscrews by splinting, placement of the miniscrew in the midpalatal suture, patient’s age (especially >15 years), and operator’s skill were factors influencing the clinical success of orthodontic miniscrews in the palate.
Since the introduction of implants as absolute anchorage in orthodontic treatment, various types of tooth movement without patient compliance have become possible with newly developed miniscrews.
Of the possible placement sites for miniscrews, the midpalatal area has been reported to be appropriate. The midpalatal suture is a highly dense structure with sufficient bone height up to the cresta nasalis, and vertical bone support is somewhat higher (at least 2 mm) than is apparent on cephalograms. The midpalatal area within 1 mm of the midsagittal suture is composed of the thickest bone available in the whole palate, and the thickness of soft tissues in the midpalatal area is uniformly 1 mm posterior to the incisive papilla, ensuring biomechanical stability of the miniscrews. There are no roots, nerves, or blood vessels to complicate the placement of surgical miniscrews, and there is no need for additional surgery because of their easy removal. Miniscrews have been placed in the midpalatal suture area of adults, and the parapalatal area in adolescents to prevent possible developmental disturbances of the midpalatal sutures. This is because the transverse growth of the midpalatal suture continues up to the late teens and is not fused completely even in adults.
Various attempts to use implants as absolute anchorage in the midpalatal suture area have been made. Now, midpalatal miniscrews are used for retraction of maxillary anterior teeth, intrusion, distalization, and protraction of maxillary posterior teeth, making it possible to produce movements that were, at best, difficult with conventional orthodontic treatment strategies.
The purpose of this study was to investigate the success rate of midpalatal miniscrews used as orthodontic anchorage for various types of tooth movements and factors affecting clinical success.
Material and methods
The subjects were 128 patients (101 female, 27 male; age range, 8.1-56.2 years; mean age, 23.4 ± 8.0 years), who received miniscrews for orthodontic anchorage in the midpalatal area. All miniscrews were placed by 1 doctor (S.H.K.) at the Department of Orthodontics, Samsung Medical Center, Seoul, Korea, between 1999 and 2005. The patients were informed about the possibilities of inflammation around and loosening of the miniscrews.
A total of 210 miniscrews were placed without flap elevation under local anesthesia. They were placed in the midpalatal sutures and, sagittally, between the mesial and distal aspects of the maxillary first molar. In adolescents, miniscrews were placed in the parapalatal area instead of the midpalatal areas to prevent possible damage to the developing sutures. An orthodontic force was applied immediately with elastomeric modules (power chain), and they were replaced every 3 weeks.
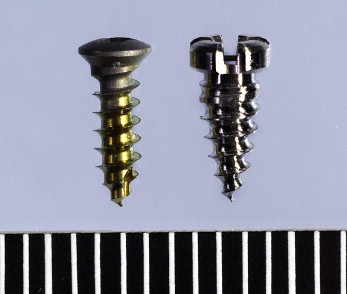
Two types of self-drilled miniscrews of the same length but different diameters were used ( Fig 1 ). One was a surgical miniscrew (diameter, 1.5 mm; length, 5.0 mm; KLS-Martin, Jacksonville, Fla) that oral surgeons usually use for fixation of bone fragments. The other was especially designed (diameter, 2.0 mm; length, 5.0 mm; Orthoplant, Biomaterials Korea, Seoul, Korea) and developed for orthodontic anchorage at the midpalatal area. Its head diameter was larger (4.0 mm) so that it provided a wide contact area between its head and a screw-supported bonded sheath (S-sheath), generating higher bonding strength sufficient to resist heavy orthodontic forces. The sheath was custom-made with a normal lingual sheath welded onto metal mesh.
Although some patients were treated with 1 miniscrew as orthodontic anchorage, most patients, especially adolescents and young adults, were treated with 2 miniscrews splinted together to ensure stability. The S-sheath was used because a heavy orthodontic force was needed to control several maxillary posterior teeth simultaneously. Splinting was done by simply bonding the S-sheath on the top of 2 miniscrews with flowable composite resin. After placing the miniscrews, 500 to 800 g of force was applied initially for various types of tooth movement: distalization, mesialization, intrusion, or retraction of anterior teeth, either singly or in combination. Elastomeric chains generally lose 50% to 70% of their initial force during the first day of load application and, at 3 weeks, retain only 30% to 40% of the original force. Therefore, we believed that 250 to 400 g might be loaded over 3 to 7 teeth after force degradation of the elastomers.
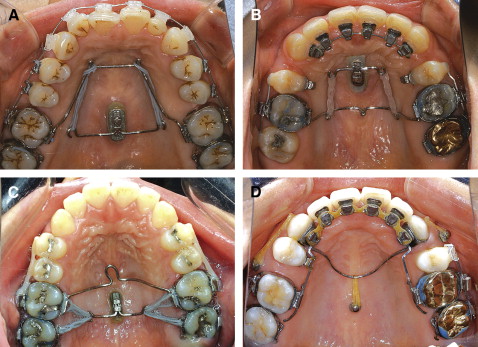
Figure 2 shows the orthodontic mechanics for some types of tooth movements by single or splinted miniscrews with or without an extension arm: distalization of maxillary molars, mesialization of maxillary molars, intrusion of maxillary molars, and retraction of anterior teeth.
The procedure was regarded as a clinical success when a miniscrew remained without loosening until it had accomplished its purpose. To examine the factors affecting the clinical success of midpalatal miniscrews for orthodontic anchorage, 10 clinical variables were investigated: operator’s learning curve (determined by calculating the success rate of miniscrews placed by the operator over 4 time periods of 18 months each), sex, age, area (midpalatal or parapalatal), total treatment period with miniscrews, splinting (single screw vs joined screws), diameter of miniscrew (1.5 vs 2.0 mm), types of tooth movements (distalization, mesialization, intrusion, retraction of anterior teeth, and combinations), and variables representing sagittal and vertical skeletal relationships (ANB, FMA, and Sn-GoGn). In previous studies, there was no evaluation of the clinician’s skill as a factor influencing success rates. Therefore, this study included an evaluation over time of whether the operator’s increasing experience with the procedure was a factor that affected the stability of miniscrews.
Statistical analysis
Success rates related to the numbers of subjects and miniscrews were calculated. The success rate was also presented for each category of clinical variable. A continuous clinical variable was categorized to provide the success rate. Logistic regression analysis was used to examine the influence of each of 10 clinical variables (categorical variables and continuous variables without categorization) on success. Multiple logistic regression analysis was also used to investigate the influence of each variable when the effects of other variables were controlled. The odds ratio (OR) for each factor was also calculated.
Results
Fifteen of the 128 patients had at least 1 miniscrew failure, for a success rate of 88.20%. Eighteen of the 197 miniscrews failed, for a success rate of 90.80%. The average time after placement for miniscrew failure was 3.5 months.
Logistic regression analysis showed no significant association between the success rate and each of following variables: sex, total period of treatment with miniscrews, diameter of miniscrew, types of tooth movement, and variables representing sagittal and vertical skeletal relationships (ANB, FMA, and Sn-GoGn).
Six of 51 miniscrews placed in 27 male patients were recorded as failures, for a success rate of 88.2%. In 101 female patients, 12 of 146 miniscrews failed, representing a success rate of 91.8%. There was no statistically significant difference in the success rates between the sexes (OR = 0.70; P = 0.4517).
The total period of treatment with miniscrews varied according to the purpose of orthodontic treatment. Although some patients were treated for less than 6 months with miniscrews, other treatments lasted more than 18 months. When a miniscrew failed before it achieved its purpose, it was replaced. In these cases, the total period of treatment with miniscrews was calculated by the sum of the periods during which the 2 miniscrews were loaded. In the group of patients with relatively short treatments (<6 months), 3 of 11 miniscrews failed, for a success rate of 72.7%. In the group with longer treatments (>18 months), some patients needed more than 1 miniscrew because of the early loss of the first miniscrew, and 11 of 111 miniscrews failed, for a success rate of 90.1%. Even though the difference in success rates between the groups with shorter and longer treatment periods (72.7% and 90.1%-95.1%, respectively) was high, there was no statistical significance between the treatment period and the success rate (OR = 0.93; P = 0.2386).
Similarly, the success rate for miniscrews with a 2.0-mm diameter (91.9%) was slightly higher than for those with a 1.5-mm diameter (89.0%), but the diameter of the miniscrews was not a significant factor.
With the midpalatal miniscrews, various kinds of tooth movements could be made: distalization, mesialization, intrusion, retraction of anterior teeth, and combinations of these. Although these movements require heavy forces of over 500 g, the success rates varied from 88.7% to 96.0%; there were no statistically significant differences.
The success rate according to the ANB difference representing sagittal skeletal relationships varied from 89.1% (Class I) to 97.1% (Class III), but there was no significant association between the ANB value and the success rate (OR = 1.05). In patients whose FMA and Sn-GoGn represented vertical skeletal relationships, those with high angles had high success rates of 97.4% (FMA) and 97.1% (Sn-GoGn), but there were also no significant associations (OR = 1.03 [FMA)]; 1.02 [Sn-GoGn]).
There were significant associations between the success rate and the following variables: operator’s learning curve, age, area, and splinting. The operator’s learning curve, which indicated his skill or experience over time, had a significant association with the success rate; the longer his learning experience, the higher the success rate (OR = 1.60; P = 0.0132). During the first 18 months, when the operator was not accustomed to the procedure for placing miniscrews in the palate, 9 of 36 miniscrews failed, a success rate of 75%. This was much lower than the rates of later periods (91.2%-97.9%); the success rate increased to more than 95% after the third period of 18 months.
Age was also associated with the success rate, and the logistic regression analysis showed that older patients had higher success rates (OR = 1.01; P = 0.0249). Notably, in the group of patients less than 15 years of age, 9 of 31 miniscrews failed, for a success rate of 71.0%, which was much lower than rates for the older groups (92.9%-100%).
In the parapalatal area, 5 of 24 miniscrews failed, whereas in the midpalatal area, only 13 of 173 failed. Thus, the miniscrews in the parapalatal area showed a significantly lower success rate (79.2%) than those in the midpalatal area (92.5%) (OR = 2.77; P = 0.0426).
Splinting the 2 miniscrews produced a higher success rate (95.9%) than use of 1 miniscrew (82.4%) (OR = 0.23; P = 0.0033), and splinting was also the only clinical variable that showed a significant association with the success rate (OR = 0.09; P = 0.013) after controlling for the effects of the other variables ( Table ).
| Logistic regression | Multiple logistic regression | ||||||
|---|---|---|---|---|---|---|---|
| Clinical variable | Miniscrews (n) | Loosened miniscrews (n) | Success rate (%) | OR | P value | OR | P value |
| Operator’s learning curve (mo) | 1.60 | 0.0132 | 1.33 | 0.2911 | |||
| First 18 | 36 | 9 | 75.0 | ||||
| Second 18 | 68 | 6 | 91.2 | ||||
| Third 18 | 47 | 1 | 97.9 | ||||
| Fourth 18 | 46 | 2 | 95.7 | ||||
| Sex | 0.4517 | 0.7164 | |||||
| Male | 51 | 6 | 88.2 | 0.70 | 0.71 | ||
| Female | 146 | 12 | 91.8 | 1.00 | 1.00 | ||
| Age (y) | 1.01 | 0.0249 | 3.23 | 0.1269 | |||
| <15 | 31 | 9 | 71.0 | ||||
| <20 | 32 | 0 | 100.0 | ||||
| <30 | 112 | 8 | 92.9 | ||||
| >30 | 22 | 1 | 95.5 | ||||
| Area | 0.0426 | 0.2716 | |||||
| Midpalatal | 173 | 13 | 92.5 | 2.77 | 3.23 | ||
| Parapalatal | 24 | 5 | 79.2 | 1.00 | 1.00 | ||
| Total treatment period using miniscrews (mo) | 0.93 | 0.2386 | 0.94 | 0.4569 | |||
| <6 | 11 | 3 | 72.7 | ||||
| 6-12 | 41 | 2 | 95.1 | ||||
| 12-18 | 34 | 2 | 94.1 | ||||
| >18 | 111 | 11 | 90.1 | ||||
| Splinting | 0.23 | 0.0033 | 0.09 | 0.013 | |||
| Single | 74 | 13 | 82.4 | ||||
| Splint | 123 | 5 | 95.9 | ||||
| Miniscrew diameter (mm) | 0.74 | 0.4975 | 0.33 | 0.2674 | |||
| 1.5 | 73 | 8 | 89.0 | ||||
| 2.0 | 124 | 10 | 91.9 | ||||
| Tooth movements | 0.7875 | 0.6193 | |||||
| Distalization | 55 | 4 | 92.7 | 0.55 | 0.56 | ||
| Mesialization | 10 | 1 | 90.0 | 0.40 | 0.28 | ||
| Intrusion | 36 | 4 | 88.9 | 0.36 | 0.39 | ||
| Retraction of anterior teeth | 71 | 8 | 88.7 | 0.36 | 0.57 | ||
| Combination | 25 | 1 | 96.0 | 1.00 | 1.00 | ||
| Sagittal skeletal relationship | |||||||
| ANB (°) (mean) | 1.05 | 0.5302 | 1.16 | 0.2195 | |||
| Class I (3.28) | 128 | 14 | 89.1 | ||||
| Class II (7.42) | 35 | 3 | 91.4 | ||||
| Class III (−1.91) | 34 | 1 | 97.1 | ||||
| Vertical skeletal relationship | |||||||
| FMA (°) (mean) | 1.03 | 0.3814 | 1.08 | 0.4444 | |||
| Low angle (20.16) | 36 | 4 | 88.9 | ||||
| Middle angle (29.5) | 122 | 13 | 89.3 | ||||
| High angle (39.8) | 39 | 1 | 97.4 | ||||
| Sn-GoGn (°) (mean) | 1.02 | 0.5129 | 1.02 | 0.8381 | |||
| Low angle (28.3) | 30 | 3 | 90.0 | ||||
| Middle angle (38.0) | 138 | 14 | 89.9 | ||||
| High angle (48.4) | 34 | 1 | 97.1 | ||||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


