8
Operative treatment of dental caries in the primary dentition
M.S. Duggal and P.F. Day
Chapter contents
8.4 Diagnosis and treatment planning
8.5 Durability of restorations
8.5.1 Conventional restorative materials
8.7 Operative treatment of primary teeth
8.8 Pulp therapy in primary teeth
8.8.1 Pulpal response to caries progression and the assessment of pulpal health
8.8.2 Treatment options for the inflamed pulp
8.8.3 Hall crown or no caries removal
8.8.4 Indirect pulp capping (IPC)
8.8.5 Direct pulp capping (DPC)
8.8.8 Management of non-vital and abscessed primary molars—the pulpectomy technique
8.9 Treatment of a child with high caries rate
8.1 Introduction
While there is no doubt that the best way to tackle the problem of dental caries is through an effective programme of prevention as outlined in the previous chapters, it is unfortunate that many children still suffer from the disease and its consequences. Hence there is a need to consider operative treatment to prevent the breakdown of the dentition. As discussed in earlier chapters, there are a number of different techniques and philosophies in treating dental caries. This chapter will concentrate mainly on the methods of complete caries removal. Research to support different philosophies, techniques, and materials frequently lacks evidence from randomized controlled trials, considered as the gold standard. Consequently, lower levels of evidence are used to support different techniques. More importantly dentists need to be skilled in different techniques and philosophies to ensure that appropriate care is provided to each and every child.
The removal of caries is not a new concept for the treatment of dental decay. Over the years the treatment of dental caries in children has been discussed and many attempts have been made to rationalize the management of the disease. Writing more than 150 years ago, Harris (1839) was one of the first to address the problem of restoring the primary dentition. Even in those days he was emphasizing the importance of prevention by good toothbrushing. Caries could be arrested by ‘plugging’, but from his description he obviously found treatment for the young patient difficult and not as successful as in adults. However, he did emphasize the importance of looking after children’s teeth: ‘If parents and guardians would pay more attention to the teeth of their children, the services of the dentist would much less frequently be required’, and, ‘Many persons suppose that the teeth, in the early periods of childhood, require no attention, and thus are guilty of the most culpable neglect of the future well-being of those entrusted to their care’. Unfortunately, this statement still applies today.
Caries removal can be a stressful experience for the child, the parent, and the dentist. Therefore it is important that there is a positive health gain from any treatment that is provided. In this chapter we aim to outline the rationale for providing operative treatment, to give advice on the selection of appropriate ways of providing care, and to describe a few of the more useful treatment methods.
8.2 Philosophy of care
Any dental care provided for children should promote positive dental experiences, which in turn would promote positive dental attitudes in their later lives.
The importance of the history and examination cannot be underestimated. It is at this consultation that the dentist attempts to ascertain the motivation of the child and parent, the extent of decay, the age of the patient and the time that teeth are expected to survive until exfoliation, any symptoms associated with the decay, and the response of the underlying dental pulp. With this information the dentist can start to formulate a treatment plan and philosophy which is appropriate for each child.
When faced with a tooth that has caries, the first decision has to be whether it does in fact require treatment. It may be felt that the caries is so minor and prevention so effective that further progress of the lesion is unlikely. Less rationally, it may be felt that a carious tooth with a non-vital pulp is unlikely to cause great problems and may be left to its own devices. There has been much discussion in the UK on whether most carious primary molars need to be restored at all! In the authors’ view there is no doubt that untreated caries in the primary dentition causes abscesses, pain, and suffering in children. This can then need hospital admission and invasive treatment, sometimes under general anaesthesia, whereas a simple restoration, at the time when the caries was diagnosed, would have prevented this extremely distressing episode for the child. Therefore it is essential for all dentists involved in the care of young children to learn restorative techniques that give the best results in primary teeth, and this should always be alongside excellent preventive programmes. This chapter is devoted to the discussion of such techniques. Good-quality restorative care (Fig. 8.1), as and when caries is diagnosed, would also obviate the need for extractions of primary teeth under general anaesthesia for thousands of children, particularly in the UK. A treatment philosophy which the authors believe is effective in the management of caries in children is shown in Table 8.1.
8.3 Remove, restore, or leave
There are certain situations where the clinician might decide not to carry out invasive restorative procedures in primary teeth and instead use a rigorous preventive approach. Such an approach can be justified where it is likely that remineralization would occur or the tooth would be maintained in a state free from pain or infection until exfoliation. It has been proposed (Pitts and Longbottom 1995) that it should be possible to divide lesions into those for which preventive care is advised (PCA) and those for which operative care is advised (OCA). More work is required on this concept, but the following sections discuss conflicting reasons to treat or not to treat particular carious lesions.
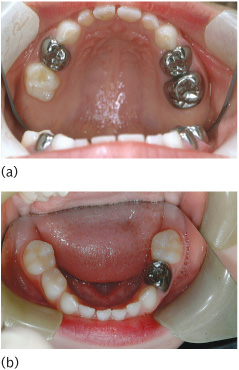
Figure 8.1 A well-restored primary dentition in a child: (a) upper arch; (b) lower arch. High-quality restorative care is supplemented with prevention in the form of sealants placed in other molars deemed to be susceptible to future carious attack.
8.3.1 Reasons not to treat
These can be divided into several distinct categories.
1. The damage done by treatment to:
(a) The affected tooth. However conservative the technique, it is inevitable that some sound tooth tissue has to be removed when operative treatment is undertaken. This weakens the tooth and makes it more likely that problems such as cracking of the tooth or loss of vitality of the pulp may occur in the future. (See Key Point 8.1.)
 Key Point 8.1
Key Point 8.1
Every time that a restoration is replaced more sound tissue has to be removed, putting the tooth at further risk.
(b) The adjacent tooth. It is almost inevitable when treating an approximal lesion that the adjacent tooth will be damaged. The outer surface has a far higher fluoride content than the rest of the enamel so that even a slight nick of the intact surface will remove this reservoir of fluoride. Additionally, it has been shown that early lesions that remineralize are less susceptible to caries than intact surfaces, and these areas of the tooth are all too easily removed when preparing an adjacent tooth. The risk for an adjacent tooth has been demonstrated in the literature. (See Key Points 8.2.)
 Key Points 8.2
Key Points 8.2
• Early lesions that remineralize are less susceptible to caries.
• When preparing an interproximal cavity take great care not to damage the adjacent tooth.
Table 8.1 Five-point treatment philosophy for the provision of high-quality dental care for children
(c) The periodontal tissues. Dental treatment can cause both acute and long-term damage to the periodontium. It is virtually impossible to avoid damaging the interdental papillae when treating approximal caries. The papillae can be protected by using rubber dam and/or wedges, and the tissues will heal fairly rapidly if well-fitting restorations are placed, but long-term damage can be more critical. Many adults can be seen to be suffering from overenthusiastic treatment of approximal caries in their youth, and while the relative importance of poor margins compared with bacterial plaque can be debated, the potential damage from approximal restorations is sufficient reason to avoid treatment unless a definite indication is present. Well-fitting stainless steel crowns in the primary dentition rarely cause gingivitis. However, when the same material is used for first permanent molars gingivitis is a common finding in late adolescence.
(d) The occlusion. Poor restoration of the teeth can, over time, lead to considerable alteration of the occlusion. It is tempting when restoring occlusal surfaces to leave the material well clear of the opposing teeth to avoid difficulties, or to be unconcerned if the filling is slightly ‘high’. However, this can allow the teeth to erupt into contact again or the interocclusal position to change and alter the occlusion. Often this is felt to be of little concern, but there are a large number of adults where the cumulative effect of many poorly restored teeth has severely disturbed the occlusion, thus making further treatment difficult, time-consuming, and expensive. The effect of occlusal rearrangement in the primary dentition appears to be less of an issue. The Hall technique of placing stainless steel crowns is one such example where the occlusion is left high. Currently, medium-term studies appear to show no detrimental effect with adjacent teeth over-erupting to accommodate the ‘high’ crown, although a significant amount of research is still required to show that this is indeed the case.
2. The difficulty of diagnosis. It is well known that it is difficult to diagnose dental caries accurately. Even when coarse criteria such as those developed for the UK Child Dental Health Surveys are used, there is variation between examiners. It is not just variations between examiners that need to be considered; there are also differences between the same examiner on different occasions. The implications need to be considered in relation to the decision to treat or not. The role of bitewing radiographs in the primary dentition leads to an approximate doubling in diagnostic yield for proximal caries.
3. The slow rate of caries attack. Caries usually progresses relatively slowly, although some individuals will show more rapid development than others. The majority of children and adolescents will have a low level of caries and progress of carious lesions will be slow. In general, the older the child at the time that the caries is first diagnosed, the slower the progression of the lesion. However, a substantial group of children will have caries that develops rapidly. This rate of caries attack will also determine how frequently bitewing radiographs in the primary and mixed dentition should be taken for children.
4. The fact that remineralization can arrest and repair enamel caries. It has long been known that early smooth-surface lesions are reversible. In addition, it is now accepted that the chief mechanism whereby fluoride reduces caries is by encouraging remineralization, and that the remineralized early lesion is more resistant to caries than is intact enamel. Although it is difficult to show reversal of lesions on radiographs, many studies have demonstrated that a substantial proportion of early enamel lesions do not progress over many years. (See Key Point 8.3.)
 Key Point 8.3
Key Point 8.3
When no plaque is present on a tooth, the caries process will stop. This emphasizes the importance of good brushing and flossing of proximal surfaces.
5. The short life of dental restorations. Surveys of dental treatment have often shown a rather disappointing level of success. In general, 50% of amalgam restorations in permanent teeth can be expected to fail during the 10 years following placement. Some studies have shown an even poorer success rate when looking at primary teeth, and this has been put forward as a reason for not treating these teeth. In one study, 61% of restorations placed in general practice had failed within a 23-month period.
8.3.2 Reasons to treat
1. Adverse effects of neglect. The fact that the treatment of approximal caries can cause damage to the affected tooth, the adjacent tooth, the periodontium, and the occlusion is a valid reason to think twice before putting bur to tooth. But a case can equally well be made that the neglect of treatment could cause as much or more damage. Lack of treatment can, and all too often does, lead to loss of contact with adjacent and opposing teeth, exposure of the pulp, resulting in the development of periapical infection, and/or loss of the tooth. At worst, the child may end up having a general anaesthetic for the removal of one or more teeth in combination with an associated facial swelling and several days in hospital on intravenous antibiotics, a process which has a significant morbidity. There is the occasional case of a child who develops lethal complications from their untreated decay.
2. Unpredictability of the speed of attack. While it is true that the rate of attack is usually slow, it is quite possible for the rate in any one individual to be sufficiently rapid that any delay in treatment would not then be in the best interests of the child.
3. Difficulty in assessing whether a lesion is arrested. Because of the normal slow rate of attack it is difficult to be sure if a lesion is arrested or merely developing very slowly. It is true that remineralization will arrest and repair early enamel lesions, but there is, in fact, little evidence that remineralization of the dentine or the late enamel lesion is common.
4. Success when careful treatment is provided. The majority of published studies show that class II amalgam or glass ionomer restorations in primary teeth have a poor life expectancy, but this is not the experience of the careful dentist. Some of these dentists have published their results, which show that the great majority of their restorations in primary teeth survive without further attention until they exfoliate. The treatment procedures used are not particularly difficult compared with others that dentists attempt on adults, and it is difficult to avoid the conclusion that the reasons for poor results in some studies are due to poor patient management and lack of attention to detail. It should be the aim of the profession to develop better and more effective ways of treating the disease, rather than throwing our hands up in surrender and expressing frustration just because so many restorations for primary teeth are placed without adherence to good principles of restorative dentistry.
5. Early treatment is more successful than late treatment. Small restorations are more successful than large restorations, and therefore if a carious lesion is going to need treatment it is better treated early rather than late. This was the rationale behind the early suggestions of a ‘prophylactic filling’ for pits and fissures, and for the modern versions in the form of fissure sealants and preventive resin restorations. The fact that small restorations are often more successful makes for difficult decisions when the management of caries involves preventive procedures which need both time to work and time to assess whether they have been effective.
8.3.3 Remove or restore
Once a decision has been made to treat a carious primary tooth a further decision has to be made as to whether to remove or restore it. This decision should take into account the following:
1. The child. Each child is an individual and treatment should be planned to provide the best that is possible for that individual. Too often treatment is given which is the most convenient for the parent or, more likely, the dentist. Is it really in the best interest of the child to remove a tooth which could be saved? A number of studies have identified tooth extraction under local anaesthetic as a significant cause of dental anxiety in children, which is not the case for restorative care. Furthermore, in the UK general anaesthesia is still widely used for removing the teeth of young children despite the risks of death, its unpleasantness, and the cost involved. (See Key Point 8.4.)
 Key Point 8.4
Key Point 8.4
Treat the child—not the convenience of parents or dentist.
2. The tooth. It is not usually in a child’s interest for a permanent tooth to be removed. However, if the pulp of a carious permanent tooth is exposed, a considerable amount of treatment may be required to retain it, and the prognosis for the tooth would still be poor. Therefore it may be in the child’s long-term interest to lose it and to allow another tooth to take its place, either by natural drift or with orthodontic assistance. Primary teeth are often considered by parents and some dentists as being disposable items because there comes a time when they will be exfoliated naturally. However, it is an unusual child who thinks the same way! Loss of a tooth before its time has a considerable significance in a child’s life. Losing a tooth early gives a message to the child that teeth are not valuable and not worth looking after. It can then be difficult to persuade a child to care for his/her teeth. Well-restored primary dentition can be a source of pride to young children and an encouragement for them to look after the succeeding teeth. It is usually more important, and fortunately rather easier, to save and restore a second primary molar than a first primary molar. While anterior teeth might be less important for the maintenance of space, their premature loss can cause low esteem in both child and parent.
3. The stage of the disease. It is easier for both child and dentist to restore teeth at an early stage of decay. Later, the pulp may become involved and subsequent restoration difficult, making loss of the tooth more likely.
4. The extent of the disease. Requirement of treatment for a large number of teeth may put a strain on a young child and, less importantly, on the parent and dentist.
The prevalence of caries in children is significantly less than it was 20 years ago, and it would be good to think that the dental profession would be able to provide effective restorative care for those who are still unfortunate enough to suffer from dental caries. Unfortunately, the care index (e.g. where teeth have been restored or extracted) is decreasing rather than increasing, suggesting that the opposite is true.
8.4 Diagnosis and treatment planning
This was discussed in Chapter 3 and will be only briefly outlined here. As stated above, the treatment of carious teeth should be based on the needs of the child. The long-term objective should be to help the child reach adulthood with an intact permanent dentition, no active caries, as few restored teeth as possible, and a positive attitude to their future dental health. If restorations are required, they should be carried out to the highest standard possible in order to maximize longevity of the restoration and avoid re-treatment prior to exfoliation.
8.4.1 Diagnosis
An accurate diagnosis of dental caries is important in the management of the primary dentition. The enamel of the primary tooth is thin compared with that of the permanent teeth and caries progresses quickly through it into the dentine, especially at the proximal area below the contact point, making an early diagnosis paramount. When caries is still confined to the enamel, preventive measures stand a chance of halting and reversing the lesion as discussed in Chapter 6.
Pulpal involvement
Once the caries is into the dentine, removal of the carious tissue and restoration of the tooth is required. Assessment of pulpal health both clinically and radiographically is essential. Caries can progress very rapidly through the primary dentine with early pulpal involvement. Because of the wide contact point in primary molars, clinical diagnosis is difficult when early dentinal caries is present. The collapse of the marginal ridge occurs once dentinal caries is well established. Research has shown that once the marginal ridge of a primary molar has broken away, the pulp of the tooth is significantly inflamed (Fig. 8.2).
Radiographs
The importance of radiographs for the diagnosis of caries in the primary dentition cannot be overemphasized (Fig. 8.3). As mentioned earlier, many early lesions may be halted or reversed by a rigorous preventive programme, but this depends on early diagnosis. While several techniques for caries diagnosis are available, bitewing (BW) radiography is by far the most acceptable and is widely available for use in general practice. Radiographs should form a routine part of any dental examination, and it is necessary to repeat radiographs for dental caries diagnosis at suitable intervals. The intervals that are appropriate to children vary according to caries risk. After an initial examination and BW radiographs, a second series should be taken within 12–24 months if the child is caries free but at 6–12 months if caries is active. Once it has been established that a child remains caries free, the interval between BWs can be increased to 24 months or even longer. However, if active caries remains a problem, 6-monthly intervals between BWs are necessary. (See Key Point 8.5.)

Figure 8.2 The marginal ridges of both the lower left first and lower right second primary molars have been involved in the carious process. The pulp in these teeth is likely to be inflamed.
 Key Point 8.5
Key Point 8.5
Destruction of the marginal ridge of a primary molar by caries indicates probable pulpal involvement.
8.4.2 Treatment planning
Treatment planning includes consideration of:
• the motivation of the child and parent, and their likely compliance with the preventive plan suggested;
• the extent of decay and the surfaces involved;
• the age of the patient and time that teeth are expected to survive until exfoliation;
• any symptoms associated with the decay;
• the health of the underlying dental pulp.
With this information the dentist can start to formulate a treatment plan and philosophy of care which is appropriate for the child. A logical treatment plan should be made which usually involves treating a quadrant of the mouth at a time. It used to be felt that multiple short visits placed least stress on a child, particularly if he/she was under 6 years of age. However, the most important aspect of child management is to gain the confidence of the child and make sure that there is as little discomfort as possible. Restorative care must be conducted with good pain control and management of a child’s behaviour. Therefore local analgesia is mandatory, and is easily performed these days with topical analgesia, fine-gauge needles, and short-acting local analgesic agents.
Where an initial stabilization phase is planned to gain the confidence of the child and buy time for cooperation to develop, this should be clearly explained to the parents. No doubt, the least interventionist approach can be the correct one for some children, but it should be integrated within a treatment plan which is best in the long-term interest of the child and not an easy way out for the dentist. If this predisposes the child to repetitive treatment, and worse still pain, abscesses, and extractions under general anaesthesia, then it should be rejected in favour of comprehensive care using restorative techniques, such as those described in this chapter. A number of other clinical tips are useful when deciding the sequence and order of care.
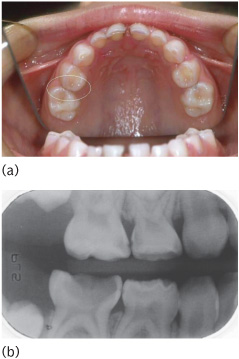
Figure 8.3 (a) A clinical examination in the upper arch gives a little clue to the presence of proximal carious lesions on both the upper right first and second primary molars. (b)However, extensive caries is evident when these are examined using BW radiographs.
Often a treatment plan should start with a relatively simple visit to introduce the child to the operative environment. This may include fissure sealant, preventive advice, or a simple buccal restoration of an anterior tooth which ideally does not require local anaesthetic.
Subsequent visits will invariably start with a simple visit using local anaesthetic (e.g. a small occlusal cavity). Where possible the order of quadrants will start with the upper arch, as this is easier to anaesthetize painlessly. If a lower quadrant is to be the starting point, consideration of using an articaine infiltration rather than a lidocaine inferior dental block may be an option as this will be a less painful injection. The presence of pain may change the order and priority of treatment visits, but wherever possible an extraction should be avoided as a first experience of operative dentistry.
Due consideration should be given to the use of a rubber dam that ensures a higher quality of restorations and can act as an aid in behaviour management. Once the tissues have been anaesthetized and the child is confident that there will be no pain, it is usually best to complete treatment on a whole quadrant. The number of visits can then be kept to a minimum and a reservoir of cooperation maintained. Where there is pulpal involvement of primary teeth, pulpotomies or pulpectomies are essential. Such teeth also need restoration with preformed metal crowns which should be placed on the same day, where clinical skill and patient cooperation allow. Finally, in each visit one or more items of preventive advice should be focused on.
8.5 Durability of restorations
Treatment decisions ought to be based on sound scientific evidence but, unfortunately, despite the great effort that has been made providing treatment over many years, little in the way of resources has been spent on clinical research into the success or otherwise of dental treatment methods. This is especially true with regard to the primary dentition. Slowly, more and more high-quality studies are being reported for different interventions, but many recommendations are based on retrospective case series and therefore need to be treated with caution.
The choice of restoration for primary teeth is based upon the criteria described in Section 8.4.2. For example, if the marginal ridge has broken away, simple proximal restoration will fail if the extent of pulpal inflammation is not considered when the choice of material is made.
8.5.1 Conventional restorative materials
Conventional restorative materials are mainly limited in use to occlusal lesions, small proximal lesions, and cavities on anterior teeth. Where caries is more extensive or involves more than two surfaces a stainless steel crown should be the default material for posterior primary molars. The benefits and disadvantages of different plastic materials are discussed in the following paragraphs. As with all materials, the operator’s attention to detail and skill are paramount in ensuring optimal survival, no matter what restorative material is chosen.
Silver amalgam
Silver amalgam has been used for restoring teeth for over 150 years and, despite the fact that it is not tooth coloured and there have been repeated concerns about its safety (largely unfounded), it is still widely used. A recent randomized trial (New England Children’s Amalgam Trial (NECAT)) could find no difference in neuropsychological or renal complications between the use of amalgam and compomer/composite when restoring posterior primary or permanent molars. However, amalgam has been discontinued in some Scandinavian countries because of environmental concerns.
Amalgam is relatively easy to use, is tolerant of operator error, and has yet to be bettered as a material for economically restoring posterior teeth. Modern non-gamma 2 alloy restorations have been shown to have extended lifetimes in permanent teeth when placed under good conditions, and have also been shown to be much less sensitive to poor handling than tooth-coloured materials.
In clinical trials and retrospective studies, no intracoronal material has so far performed more successfully than amalgam. This finding was confirmed in the NECAT study with amalgam outperforming compomer in primary molars and composite in permanent molars.
Stainless steel crowns
These were introduced in 1950 and have gained wide acceptance in North America. They have been less popular in Europe, being seen by most dentists as too difficult to use, although in reality they are often easier to place than some intracoronal restorations (Fig. 8.4). The recent development of the Hall technique, which simplifies placement, may increase their use, even though more research is required to assess the suitability of this technique. Because the entire crown of the tooth is covered, the stainless steel crown rarely needs to be replaced owing to recurrent caries or new caries at a site distant to the original filling.
All published studies have shown stainless steel crowns to have a higher success rate than all other restorative materials in primary teeth. They are certainly the preferred treatment option for primary molars with anything other than minimal caries.
Stainless steel crowns are also advocated for hypoplastic/hypomineralized or very carious first permanent molars, where they act as provisional restorations prior to either strategic removal at age 9–12 years or later restoration with a cast crown (Fig. 8.5). Etched retained castings can now be used for the definitive restoration of permanent teeth with developmental defects without involvement of the approximal surface or gingival margin; more conservative provisional restorations than stainless steel crowns should be considered if this is intended.
Composite resin
Composite resins came on the market in the early 1970s and have been modified since then in an attempt to improve their properties. The development of acid etching at the time that these materials were introduced has ensured that they have performed reasonably well in terms of marginal seal. They are sensitive to variations in technique and take longer to place than equivalent amalgam restorations. They must be placed in a dry field (Fig. 8.6).
The long-term success of composite resins is jeopardized by their instability in water. The best materials have maximum inorganic filler levels and low water absorption, but will deteriorate over time. The longevity of composite material appears to be similar to that of RMGIC or compomer for occlusal and small proximal restorations in primary teeth. The NECAT study showed inferior results compared with amalgam for the restoration of permanent molars in a population aged 6–10 years. (See Key Point 8.6.)
 Key Point 8.6
Key Point 8.6Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


