Every instance of agenesis of a tooth represents an inborn error in dentogenesis. Just as current knowledge of metabolic and regulatory roles of essential molecules has been shaped partly by how inborn errors of their metabolism cause metabolic diseases, so too can accumulation and diffusion of knowledge of defects in dentogenesis facilitate a better understanding of craniofacial morphogenesis. On a practical level, clinicians should know the extent to which protocols for oral habilitation involving dental implants can be borrowed from our primary knowledge base and used to manage patients born with multiple malformations. This article reviews the literature relevant to the use of dental implants in patients with oligodontia secondary to chromosomal syndromes, such as it is, and illustrates the management of several of them.
In Sweden, it was estimated that 15% of children and adolescents missing eight or more permanent teeth were afflicted with a syndrome such as ectodermal dysplasia (ED). Of the 2800 syndromes listed in POSSUM, a computer-based resource that helps clinicians to diagnose syndromes in their patients, 126 syndromes are associated with anodontia or oligodontia ( http://www.possum.net.au/ ). A synthesis of available literature estimated that the most frequent syndromes associated with agenesis of teeth are the EDs and Down syndrome.
ED is a syndrome characterized chiefly by abnormalities of the tissues that originate from ectoderm, namely skin, nails, hair, and teeth ( Fig. 1 ). There are more than 150 variants of ED, with hypohidrotic ED (HED) exhibiting the most severe dental anomalies and a typical craniofacial dysmorphology, which makes it of greatest interest to dentists ( Figs. 2 and 3 ). With an incidence of 1/100,000 births, HED is a relatively common syndrome. Depending on the type of treatment required, dental care for patients with ED has a significant financial impact on patients and their families.
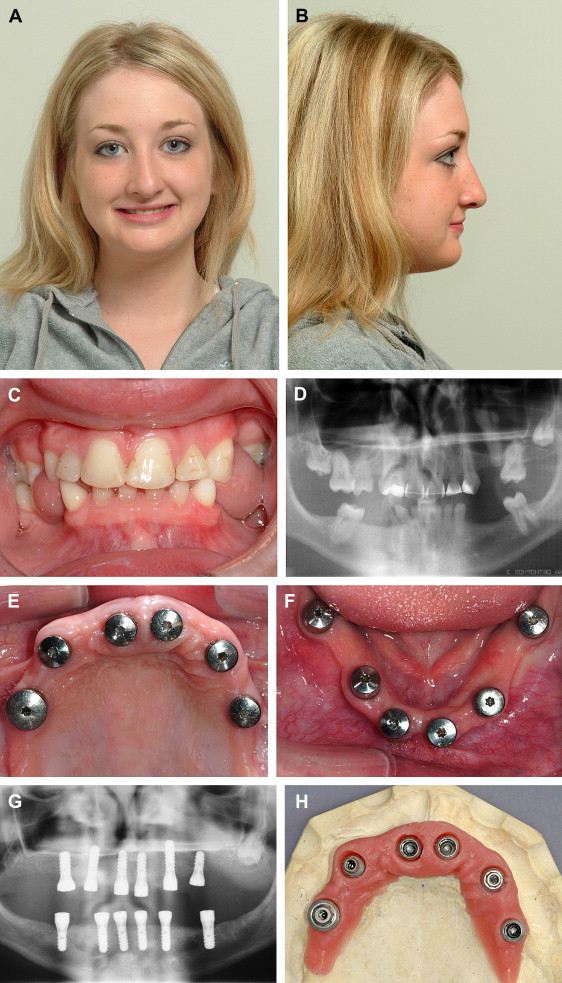
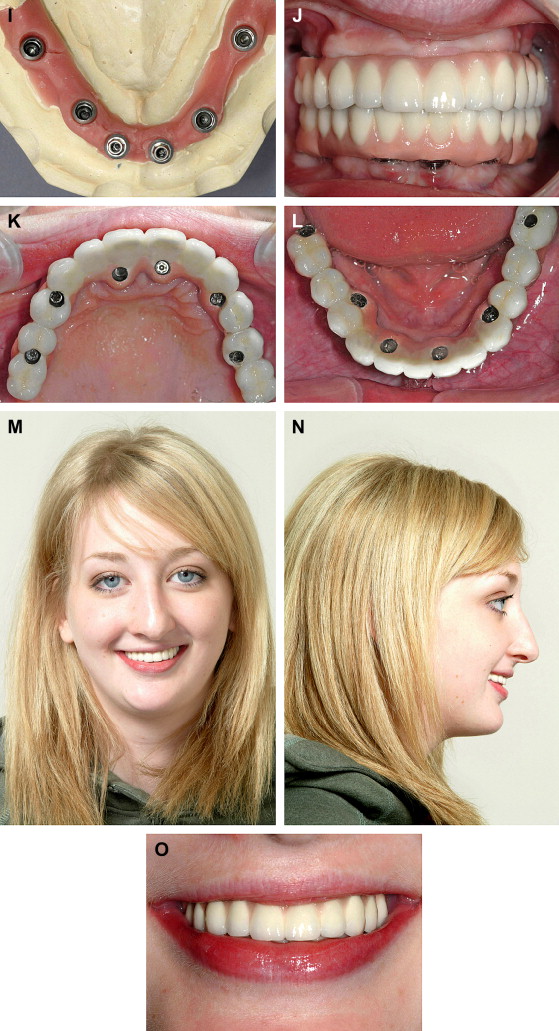

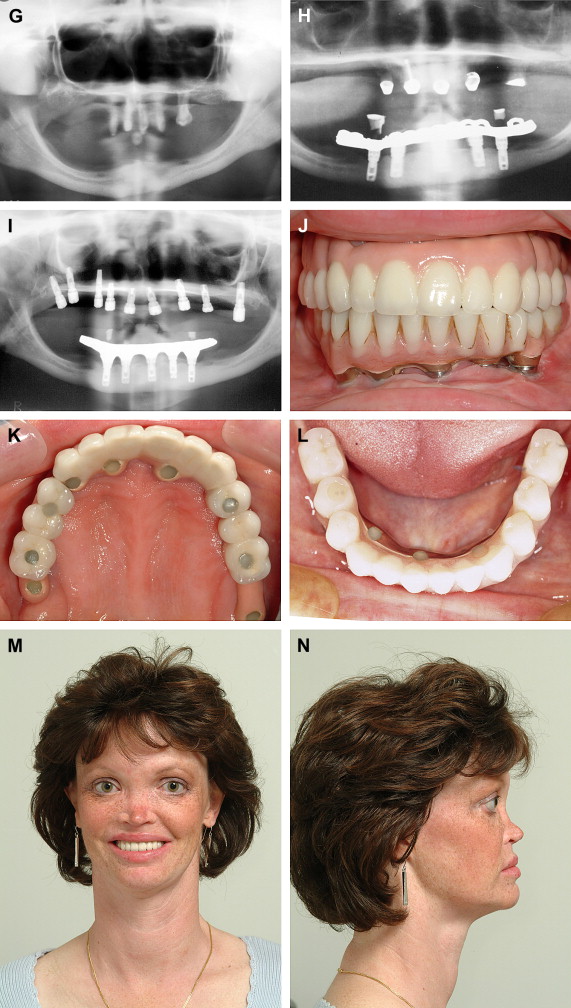
Articles in the dental implant literature tend not to distinguish among the many variants of ED ( Fig. 4 ), labeling them all simply as ED when it is likely that many—if not most—reported cases are HED. Numerous single case reports and small cohort studies in the literature describe the use of implants to support mandibular prostheses in children with ED. Since 1991, reports of single cases and small series of children with ED having been treated with implants have appeared in the literature; follow-up periods range from 0 months to 12 years and report few failure statistics. One retrospective study of 61 implants placed in 14 adolescents and young adults who were followed from 1 to 5 years reported a 67% success rate. A prospective trial of 51 patients followed for up to 78 months reported survival rates of 91% in the mandible and 76% in the maxilla. The consensus from these reports seems to be that results support the continued use of implants in young children when appropriate precautions are taken not to interfere with growth of the jaws. Research has shown that treatment with implants in patients with HED does not rescue normal craniofacial growth and development.


