Introduction
Our objectives were to evaluate and quantify upper lip soft-tissue changes in the vertical dimensions both at rest and at maximum smile, and to examine the correlation between upper labial vestibular attachment height and maxillary gingival exposure on smiling.
Methods
Seventy-two volunteers (36 men, 36 women) aged 20 to 40 (mean, 30.49 years) were recruited for this study. For each subject, 9 measurements of upper lip position and maxillary incisor crown height at rest and in maximum smile were recorded.
Results
A statistically significant sexual dimorphism was apparent in most of the measured variables. Relaxed external upper lip length was 3.1 mm shorter in the women than in the men. The mean maxillary central incisor display at rest was 1.78 mm greater in the women than in the men. A high smile line was 2.5 times more prevalent in the women. The upper lip was shortened by 30% in subjects with a high smile line compared with 23% in subjects with a low smile line.
Conclusions
The following findings were observed in subjects with a high smile pattern: (1) short upper lip length, (2) low smiling/resting upper lip length ratio, (3) inferior attachment of the upper labial vestibule, and (4) prominent upper lip vermilion.
The smile is a voluntary facial expression indicating happiness, pleasure, and greeting. According to Garber and Salama, the essentials of the esthetic smile involve the relationship between 3 primary components: teeth, lip framework, and gingival scaffold. Maxillary gingival exposure during smiling causes interest and concern among many dental practitioners and plastic surgeons. An excessive gingival display on smiling, referred to as “gummy smile,” “high lip line,” or “high smile line,” is often esthetically displeasing and considered undesirable. Several etiologic factors have been suggested in the literature, including skeletal, gingival, and muscular factors that can contribute alone or in combination to this feature. Several treatment modalities have been proposed in the literature to diminish the gingival display on smiling. In patients with clinically short anterior tooth crowns, surgical crown lengthening or gingivectomy is recommended. In other patients, whose teeth crowns are proportionally balanced, but muscular hyperactivity is suspected, injection of botulinum toxin-A to the lip elevator muscles or a lip repositioning procedure is advocated. In patients whose gingival display is excessive as a result of maxillary vertical excess, orthognathic surgery has been suggested. Some soft-tissue surgical procedures, especially lip repositioning, lack wide scientific evidence and long-term follow-ups as do some other surgical procedures; they can lead to relapse and undesirable side effects such as scar contraction.
The purposes of this study were to evaluate and quantify upper lip soft-tissue changes in the vertical dimensions at both rest and maximum smile, and to examine the correlation between upper labial vestibular attachment height and maxillary gingival exposure on smiling.
Material and methods
Seventy-two volunteers (36 men, 36 women) aged 20 to 40 years were recruited for this study. No participants had undergone any maxillofacial surgery or anterior maxillary tooth prosthodontic rehabilitation. All participants signed an informed consent, in accordance with the requirements of the ethics committee at Rabin Medical Center, Beilinson Campus, Petach Tikva, Israel.
For each subject, 9 measurements of upper lip position and maxillary incisor crown height at rest and in maximum social smiling were recorded. To reach the maximum social smile position, each subject was requested to present his or her full smile a few times, and measurements were taken when the subject successfully repeated the full smile pattern. In addition, the age and sex of each subject were recorded.
The measurements and the methods used to obtain these variables are as follows.
- 1.
Performed both at rest and maximum smiling ( Fig 1 ): (a) external upper lip length, the vertical measurement from the alar base of the nose (subnasale) to the inferior border of the upper lip (stomion superioris); (b) vermilion height, the vertical measurement from the superior border of the vermilion at the Cupid’s bow to the inferior border of the upper lip; and (c) maxillary central incisor display, the vertical measurement from the inferior border of the upper lip to the incisal edge of the left central incisor.
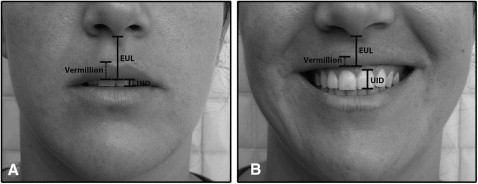
Fig 1 Vertical measurements: A, at rest; B, at smiling ( EUL , External upper lip; UID , upper incisor display). - 2.
Performed once in maximum smiling when applicable: gingival display in maximum smiling, recorded in patients whose gingival display was noticed in the maximum smile.
- 3.
Performed once at rest position: (a) internal upper lip length, the vertical measurement, with an appropriate ruler (Esthetic Lip Ruler, GDIT, Tulsa, Okla) that was slightly modified, from the labial vestibule apical to the central incisors to the inferior border of the upper lip ( Fig 2 ). During ruler placement, the upper lip was slightly elevated temporarily, and the ruler was gently pressed into the center of the upper vestibule under direct vision until the anterior nasal spine was felt. Next, the upper lip was released and gently moved to verify that it was not under exaggerated tension. Two consecutive trials were made in each subject before recording the measurement to verify the validity of the position. Measurement of hard-tissue landmarks by estimation over soft-tissue landmarks is a common and acceptable concept used in various measurements in medicine (eg, the identification of nasion and porion with a facebow). (b) Maxillary central incisor height, the vertical measurement of the clinical crown height of the maxillary left central incisor. The measurement was made under direct vision at the center of the tooth.

Fig 2 Modified lip ruler.
All measurements were recorded by the first author (H.M.) to the nearest millimeter directly on the face using a simple, small metal ruler. Internal upper lip length was measured by using the modified Esthetic Lip Ruler mentioned above.
Smile pattern was classified according to the 3 categories defined by Tjan et al, relating to the anterior maxillary tooth crown exposure at maximum smile: “low smile” displaying less than 75% of the clinical crown height of the maxillary anterior teeth, “average smile” revealing 75% to 100% of the maxillary anterior crown height, and “high smile” exposing the whole anterior maxillary crown height and a band of contiguous maxillary gingiva.
Total lip elevation length was defined (smiling maxillary central incisor display + gum exposure in smile – resting maxillary central incisor display) to quantify the vertical exposure capacity of the lip. This variable is complementary to the smiling/resting external upper lip length ratio variable in representing the upper lip’s vertical contraction during smiling. When no resting maxillary central incisor display was noticed, the total lip elevation was not calculated, since negative resting maxillary central incisor display was not measured.
Independent Student t tests were performed to assess differences between the sexes, and between subjects with and without gingival exposure in maximum smiles. One-way ANOVA was used to assess the differences between smile pattern groups. Pearson correlation analysis was used to find the relationship between the 2 variables. The level of significance was set at P ≤0.05.
Results
Means and standard deviations, derived for all measured variables of the subjects, are reported with some statistical information in Table I .
| Factor | Female (n = 36) | Male (n = 36) | Student t test |
||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (y) | 29.44 | 0.68 | 31.52 | 0.73 | −2.09 ∗ |
| Resting external upper lip length (mm) | 20.97 | 0.37 | 24.00 | 0.35 | −5.94 † |
| Resting maxillary central incisor length (mm) | 3.86 | 0.25 | 2.08 | 0.28 | 4.74 † |
| Resting vermilion/external upper lip length ratio | 0.33 | 0.01 | 0.31 | 0.01 | 1.26 NS |
| Resting internal upper lip length (mm) | 14.78 | 0.23 | 18.64 | 0.31 | −9.98 † |
| Resting internal upper lip/external upper lip length ratio | 0.71 | 0.02 | 0.78 | 0.01 | −3.25 † |
| Maxillary incisor height (mm) | 9.67 | 0.21 | 10.17 | 0.10 | −2.14 ∗ |
| Smiling external upper lip length (mm) | 15.14 | 0.30 | 17.57 | 0.37 | −5.08 † |
| Smiling maxillary central incisor display (mm) | 8.89 | 0.26 | 8.31 | 0.40 | 1.23 NS |
| Smiling/resting external upper lip length ratio | 0.72 | 0.01 | 0.73 | 0.01 | −0.47 NS |
The mean age of the whole study population was 30.49 years. The youngest subject was 20 years old, and the oldest was 39 years old. The women’s mean age was 1 year younger than the mean, and the men’s mean age was 1 year older than the mean.
A statistically significant sexual dimorphism was apparent in most of the measured variables. Relaxed external upper lip length was 3.1 mm shorter in the women than in the men ( P <0.01). The mean maxillary central incisor display at rest was 1.78 mm greater in the women than in the men ( P <0.01). The upper vermilion comprised 31% to 33% of the external upper lip length. Although it was not statistically significant, the women tended to have a higher percentage of vermilion display relative to the men. Surprisingly, the same ratio of vermilion display was preserved when smiling. The resting internal upper lip length/external upper lip length ratio represented the vertical relationship between the internal lip length, measured from the upper labial vestibule attachment, and between the upper lip external length, an external and easily identifiable anatomic landmark. This parameter was calculated to check whether internal lip insertion is a contributing factor in upper lip mobility. The level of insertion of the upper lip at the upper labial vestibule was lower in the women. The internal upper lip length/external upper lip length ratios were 71% in the women and 78% in the men ( P <0.01). Central incisor clinical crown height was 0.5 mm shorter in the women compared with the men ( P = 0.04). External upper lip length became shorter by about 27% at maximum smiling in both sexes.
High smiles, with exposure of the entire maxillary incisors and a band of gingiva, were noticed in 38.9% of the study population and were 2.5 times more prevalent in women (55.6%) than in men (22.2%). Low smiles, noticed in only 22.2% of the subjects, were 4 times more common in men (36.1%) than in women (8.3%). Table II summarizes the smile patterns by sex in the whole study population.
| Smile type | Female (%) | Male (%) | Total (%) |
|---|---|---|---|
| Low smile | 3 (8.3%) | 13 (36.1%) | 16 (22.2%) |
| Average smile | 13 (36.1%) | 15 (41.7%) | 28 (38.9%) |
| High smile | 20 (55.6%) | 8 (22.2%) | 28 (38.9%) |
| Total | 36 (100%) | 36 (100%) | 72 |
A positive, statistically significant correlation was found between smile patterns and the following parameters: resting external upper lip length, resting maxillary central incisor display, total lip elevation, and smiling/resting external upper lip length ratio. Table III summarizes some parameters in correlation to the different smile patterns. The mean external upper lip length in subjects with a low smile pattern was 2.46 mm greater than in subjects with a high smile ( P <0.01). The mean maxillary central incisor display at rest in subjects with a low smile pattern was 1.31 mm, whereas, in those with a high smile pattern, the mean maxillary central incisor display was 2.55 mm ( P <0.01). Total lip elevations were 4.2 mm in the subjects with a low smile, 6.3 mm in those with an average smile, and 7.75 mm in those with a high smile ( P <0.01). The same positive correlation was noticed between mean smiling/resting external upper lip length ratio and smile patterns. In the low smile group, external upper lip length in maximum smiling was only 23% shorter than resting external upper lip length; in the average smile group, the external upper lip was shortened by 27%, and in the high smile group by 30% ( P <0.01). Refining the results and comparing each pair of smile pattern groups, as presented in Table III , shows that most of the statistically significant differences between smile groups relied on the difference between the high and the low smile groups. Although there were differences between the high and the average smile groups, no statistical significance was found in most of the factors that were measured. These findings support the assumption that patients with a gummy smile have hyperfunction of the upper lip.
| Factor | Low smile (n = 16) |
Average smile (n = 28) | High smile (n = 28) | 1-way ANOVA | High-low Student t test |
High-average Student t test |
|||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| Resting external upper lip length (mm) | 24.00 | 2.45 | 22.58 | 2.43 | 21.54 | 2.59 | P <0.01 | P <0.01 | P = 0.13 |
| Resting maxillary central incisor display length (mm) | 1.31 | 1.14 | 3.04 | 1.60 | 3.86 | 1.72 | P <0.01 | P <0.01 | P = 0.07 |
| Total lip elevation (mm) | 4.20 | 1.32 | 6.30 | 1.54 | 7.75 | 1.80 | P <0.01 | P <0.01 | P <0.01 |
| Smiling/resting external upper lip length ratio | 0.77 | 0.05 | 0.73 | 0.07 | 0.70 | 0.08 | P <0.01 | P <0.01 | P = 0.11 |
| Resting internal upper lip length/external upper lip length ratio | 0.79 | 0.07 | 0.75 | 0.08 | 0.72 | 0.10 | P = 0.06 | P = 0.01 | P = 0.22 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


