The treatment of adult patients with severe anterior open bite frequently requires orthognathic surgery, especially when the chin is retruded severely. If a patient has multiple missing posterior teeth, it is difficult to control the occlusal plane because it is challenging to obtain anchorage during orthodontic treatment. We report on a 25-year-old woman who had a skeletal Class II malocclusion, severe anterior open bite, vertical maxillary asymmetry, and severe dental caries on her molars. There was no posterior occlusal contact between the maxillary and mandibular molars since 5 of her molars had to be extracted because of severe caries. Lingual fixed appliances and double jaw surgery were performed to treat her skeletal and dental problems, and dental implants helped restore her masticatory function. Pretreatment, posttreatment, and retention photographs demonstrate effective, esthetically pleasing, and stable treatment results.
For nongrowing patients with skeletal Class II malocclusions, there are 2 possible treatment approaches: (1) orthodontic camouflage, which consists of retraction of the maxillary incisors to improve both the dental occlusion and the facial esthetics but does not correct the underlying skeletal problem; and (2) orthognathic surgery to reposition the mandible and/or the maxilla.
Skeletal Class II problems are frequently due to mandibular deficiency or downward and backward rotation of the mandible accompanied by excessive maxillary vertical growth. Surgical treatment for these patients, therefore, consists of mandibular advancement, superior repositioning of the maxilla, or a combination of both. Jaw surgery combined with orthodontic treatment can produce a more ideal skeletal relationship than orthodontic camouflage, with the mandible more anteriorly positioned and the mandibular incisors in a more ideal position relative to the basal bone.
Treatment of anterior open bite has long been considered a challenge to orthodontists, because a successful and well-maintained result is difficult to achieve. In particular, the combination of a sagittal skeletal discrepancy and a skeletal open bite requires the highest degree of diagnostic and clinical skill to treat. The prevalence of anterior open bite ranges from 1.5% to 11% among various ages and populations. Orthodontists have many treatment options for treating open bite. High-pull headgear, posterior bite-blocks, functional appliances, multiloop edgewise archwires, mini-implants, and orthognathic surgery are possible modalities for treating an anterior open bite. However, if many of the patient’s posterior teeth have been extracted or are severely damaged, solving the patient’s occlusal and esthetic problems by orthodontic treatment alone becomes nearly impossible.
This case report describes the use of lingual fixed appliances and double jaw surgery to resolve an anterior open bite, a vertical maxillary asymmetry, and an anteroposterior skeletal discrepancy in an adult Class II patient. This 25-year-old woman had a retruded mandible and posterior teeth that were damaged by caries. Because of the severity of her caries, 5 of her molars had to be extracted, and there was no occlusal stop in the molar region. The posterior occlusion was restored with dental implants after surgical orthodontic treatment.
Diagnosis and etiology
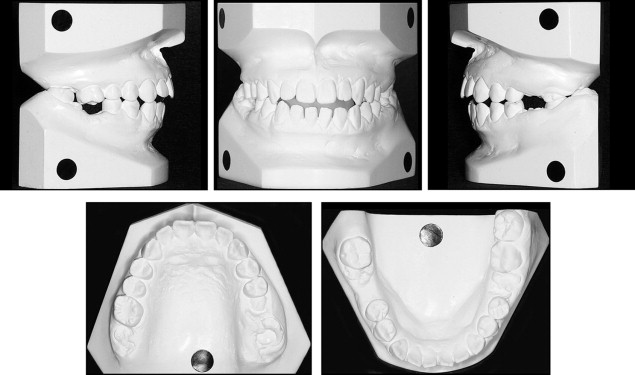
This healthy woman was referred to our clinic for orthodontic evaluation with a chief complaint of impaired occlusion because of an anterior open bite and severe dental caries. She had a retruded mandible and facial asymmetry ( Fig 1 ). Hyperactivity of the mentalis muscle was observed with the lips sealed. From the frontal view, she exhibited both occlusal plane canting and lip-line canting, but there was no dental midline deviation during smile. She was aware of her retrusive chin and lip incompetence. Intraorally, she had an anterior open bite (–2.0 mm) and multiple dental caries. Her maxillary left first and second molars, maxillary right second molar, and mandibular left and right first molars were severely damaged by dental caries. Her canine relationship was Class II on both sides ( Fig 2 ). The occlusal examination showed interdental spacing in the mandibular anterior region.
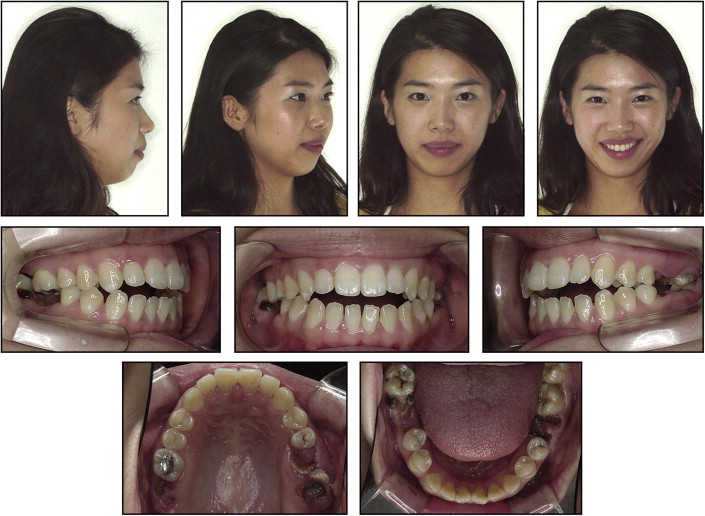
The patient did not have an unusual medical history. The functional assessment showed no limitation of movement during jaw opening and no apparent signs and symptoms of temporomandibular disorders. Her panoramic radiograph showed multiple root rests, an impacted mandibular right third molar, and distal inclination of the condylar head ( Fig 3 ). The mandibular right third molar was tipped mesially and impacted horizontally.
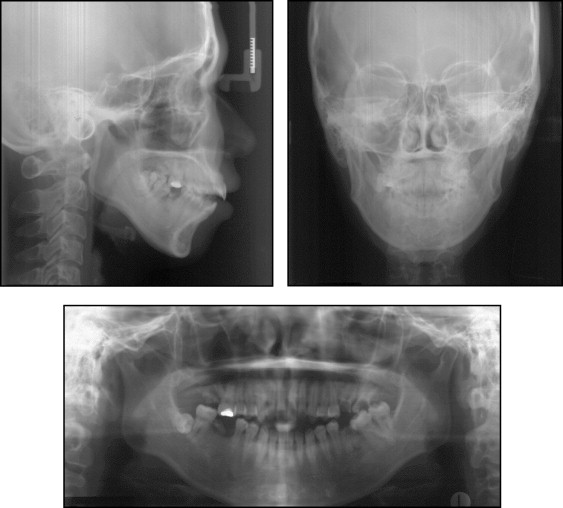
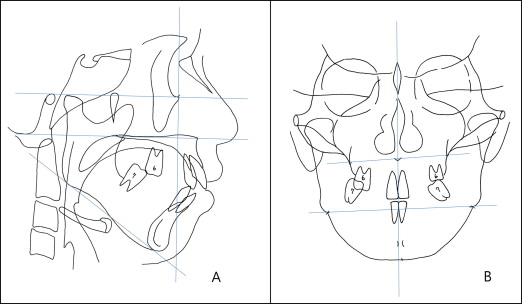
The lateral cephalometric analysis ( Fig 4 and Table ) showed a skeletal Class II relationship (ANB angle, 9.2°) caused by a retrognathic mandible (Pog to N perpendicular, –11.8 mm). Her facial pattern was hyperdivergent, as evidenced by a facial height ratio of 60.4. The maxillary and mandibular incisors were normally positioned. Posteroanterior cephalometric analysis ( Fig 4 ) showed a slight chin point deviation from the skeletal midline because of vertical maxillary asymmetry. She also had an asymmetric shape of the mandibular angle region.
| Norm ∗ | Pretreatment | Posttreatment | Postretention | |
|---|---|---|---|---|
| Bjork sum (°) | 393.3 | 399.9 | 398.5 | 398.3 |
| Facial height ratio (%) | 65.0 | 60.4 | 61.0 | 61.1 |
| ANB (°) | 2.6 | 9.2 | 4.5 | 4.2 |
| A to N perpendicular (mm) | −0.5 | 5.4 | 2.6 | 2.5 |
| Pog to N perpendicular (mm) | −2.6 | −11.8 | −1.3 | −1.1 |
| U1 to FH (°) | 113.8 | 114.9 | 112.0 | 112.2 |
| U1 to SN (°) | 105.3 | 112.8 | 108.8 | 109.1 |
| U1 to Sto′ (mm) | 2.7 | 3.0 | 0.3 | 0.2 |
| L1 to A-Pog (°) | 5.4 | 7.8 | 2.6 | 2.8 |
| IMPA (°) | 95.9 | 96.0 | 84.3 | 84.6 |
| Interincisal angle (°) | 125.4 | 111.6 | 130.8 | 130.2 |
| Nasolabial angle (°) | 98.0 | 98.5 | 97.6 | 98.0 |
| Upper lip to E-line (mm) | −1.2 | 1.4 | −1.8 | –2.0 |
| Lower lip to E-line (mm) | 0.0 | 4.3 | 0.2 | 0.0 |
| Upper occlusal plane to maxillary incisor (°) | 55.0 | 53.4 | 52.5 | 52.2 |
| Lower occlusal plane to mandibular incisor (°) | 66.0 | 66.7 | 77.5 | 77.3 |
| Upper occlusal plane to AB (°) | 94.0 | 86.5 | 93.7 | 93.9 |
| AB to FH (°) | 81.0 | 76.0 | 80.4 | 80.6 |
| FH to upper occlusal plane (°) | 12.0 | 12.5 | 15.0 | 14.8 |
| Sn′-Sto′: Sto′-Me′ | 1:1.90 | 1:1.94 | 1:1.85 | 1:1.83 |
Treatment alternatives
The first alternative was orthognathic surgery because of her skeletal discrepancy. Maxillary asymmetrical impaction with clockwise rotation, which would induce mandibular autorotation, correct the vertical asymmetry, and improve the nasolabial angle, and concurrent mandibular advancement surgery could be planned to improve her facial profile. Advancement and vertical reduction genioplasty would move the chin forward and reduce the long lower facial height. Additional mandibular angle osteotomies would be needed to correct the asymmetry of her mandibular angle region. This option would not only correct the Class II occlusal problems, but also significantly improve her facial profile.
The second option consisted of orthodontic camouflage to obtain proper overbite and overjet, and dental implants placed after orthodontic treatment. Although this treatment option would improve the occlusal relationship and obtain a positive overbite, it would not significantly improve her profile and lip competence because the change in chin position would be minimal. In addition, this option could not correct the vertical maxillary asymmetry. If there had been teeth in the molar region, orthodontic mini-implants could have helped to improve the facial profile and control the vertical maxillary asymmetry without surgical treatment. As a result, the first option was selected because the patient’s main concern was facial esthetics.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


