This report describes the orthodontic treatment of a woman, aged 34 years 2 months, with several missing teeth and atrophic mandibular first molar extraction sites. We had planned to close the spaces from the missing maxillary canines with mesial movement of the premolars and molars. In the mandibular arch, protraction of the second molars into first molar extraction sites and reduction of the mandibular incisor protrusion were performed. No miniscrews or bone plates were used. A modified helical loop was used, and it can be considered a simple and an efficient orthodontic method of closing the spaces without mesial or lingual tipping and rotation. Pleasing esthetic and functional results were achieved.
Orthodontic treatment for patients with several missing teeth is challenging. Orthodontists are often confronted with adults who have large edentulous spaces in the molar areas or need molar extractions. Adults needing comprehensive orthodontic therapy often have dental and periodontal problems that require multidisciplinary treatment approaches. Such problems include periodontal defects, missing teeth, and atrophic extraction sites.
Proffit et al described several common sequelae of missing mandibular first molars, such as tipping and drifting of adjacent teeth, poor interproximal contacts, poor gingival contour, reduced interradicular bone, and supereruption of unopposed teeth. Since the bone contour follows the cementoenamel junction, pseudopockets form adjacent to the tipped teeth. In adults, closing an extraction site with bone defects is a challenge for orthodontists. Typically, several years after the extractions, bone remodeling results in narrowing of the alveolar ridge; therefore, closure of the extraction spaces requires remodeling of cortical bone. Additionally, malocclusions in adults can be complicated by the migration of adjacent teeth into the extraction sites. Under these circumstances, functional and esthetic results might only be achieved with the combination of surgery, orthodontic treatment, and prosthodontic rehabilitation. The aim of this case report was to present the interdisciplinary treatment of an adult patient with several missing teeth, preexisting extraction spaces, and some periodontal and esthetic problems that required applied orthodontic mechanics.
Etiology and diagnosis
The patient, a woman, aged 34 years 2 months, was referred for orthodontic evaluation by her general dentist. Her chief complaints were her dissatisfaction with her smile and the spaces in the maxillary and mandibular dental arches. Her medical history showed no contraindication for orthodontic therapy. Extraoral examination showed symmetric facial structures, and lip competence could be achieved at rest with no strain. She had a slightly concave profile, and the upper lip was retruded relative to the lower lip. Her nasolabial angle was normal ( Fig 1 ).

There were no signs or symptoms of temporomandibular joint dysfunction. Mandibular movements, such as maximal opening and lateral and anterior displacement, were within normal limits. Intraoral analysis showed coincidence of the maxillary and mandibular dental midlines relative to the facial midline. Overjet was 3 mm, and overbite was 2.5 mm. A negative space discrepancy (−2 mm) was present in the mandibular incisor region. The mesiodistal width of the maxillary lateral incisors was narrowed, and the maxillary canines were not visible intraorally. Surgical extraction of the maxillary left canine was reported by the patient. The mandibular first molars and maxillary left first molar had been extracted because of extensive caries when she was an adolescent, and the alveolar ridges were atrophic and narrowed.
The edentulous spaces mesial to the mandibular second molars measured 8 mm on the right side and 7 mm on the left side. The buccolingual widths of atrophic bone were 5 mm on the right side and 4 mm on the left side. The mandibular second and third molars and the maxillary left second and third molars had tipped and drifted mesially. The mandibular third molars were present and anatomically normal ( Fig 2 ). She had a maxillary removable partial denture, but she was displeased with the esthetic appearance, and it was uncomfortable.

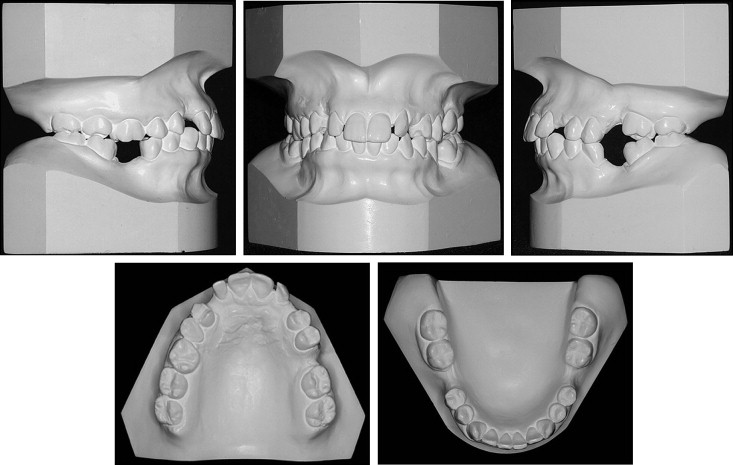
Although the first molars and maxillary canines were missing, the premolars had a Class II relationship. The intercanine width was 24 mm, and the intermolar width was 47 mm. The curve of Spee was moderate ( Fig 3 ).
The panoramic radiographs showed no caries or pathology. The maxillary right canine was dilacerated and impacted in an oblique position. The maxillary right first molar, second premolar, and lateral incisor, as well as the left central and lateral incisors, had been treated endodontically. The mesial region of the maxillary second molar had a significant periodontal bone defect ( Fig 4 ).

The cephalometric radiograph and analysis confirmed the maxillary protrusion and a well-positioned mandible (SNA, 85°; SNB, 80°). Although the ANB of 5° suggested a skeletal Class II pattern, profile variables showed that the upper lip was retruded relative to the lower lip (upper lip to S line, −4 mm; lower lip to S line, −3.5 mm). Her facial form was considered mesocephalic (GoGn to SN, 39.5°; FMA, 26.5°). Dentally, the maxillary incisors were well positioned (U1 to NA, 5 mm; U1 to NA, 23°). The mandibular incisors were protrusive (L1 to NB, 8 mm) and also proclined relative to the cranial base (L1 to NB, 29°) with a closed interincisal angle (123°) ( Fig 5 , Table ).

| Variable | Norm | Pretreatment (T1) | Posttreatment (T2) | (T2-T1) |
|---|---|---|---|---|
| SNA (°) | 82 | 85 | 85.5 | 0.5 |
| SNB (°) | 80 | 80 | 80 | 0 |
| ANB (°) | 2 | 5 | 5.5 | 0.5 |
| GoGn to SN (°) | 32 | 39.5 | 38 | −1.5 |
| FMA (°) | 25 | 26 | 26.5 | 0.5 |
| FMIA (°) | 67 | 65.5 | 69 | 3.5 |
| IMPA (°) | 88 | 88.5 | 84.5 | −4 |
| U1 to NA (°) | 22 | 23 | 9 | −14 |
| U1 to NA (mm) | 4 | 5 | 0 | −5 |
| L1 to NB (°) | 25 | 29 | 24 | −5 |
| L1 to NB (mm) | 4 | 8 | 5.5 | −2.5 |
| Interincisal angle (°) | 131 | 123 | 141 | 18 |
| Pog to NB (mm) | – | 0 | 0.5 | 0.5 |
| Upper lip to S line (mm) | 0 | −1.5 | −1 | 0.5 |
| Lower lip to S line (mm) | 0 | 0.5 | 0 | −0.5 |
Treatment objectives
- 1.
Extract the impacted maxillary right canine and obtain a Class I relationship between the maxillary premolars and the mandibular canines.
- 2.
Improve smile esthetics by aligning and leveling both dental arches, closing the space of the maxillary canines with mesial movement of the premolars and molars, and increasing the mesiodistal width of the maxillary lateral incisors.
- 3.
Prepare space for dental implants in the maxillary left first molar area.
- 4.
Protract the mandibular second molars into the first molar extraction sites.
- 5.
Improve the facial profile.
- 6.
Obtain normal overjet and interincisal guidance.
- 7.
Reduce the mandibular incisor protrusion.
Treatment objectives
- 1.
Extract the impacted maxillary right canine and obtain a Class I relationship between the maxillary premolars and the mandibular canines.
- 2.
Improve smile esthetics by aligning and leveling both dental arches, closing the space of the maxillary canines with mesial movement of the premolars and molars, and increasing the mesiodistal width of the maxillary lateral incisors.
- 3.
Prepare space for dental implants in the maxillary left first molar area.
- 4.
Protract the mandibular second molars into the first molar extraction sites.
- 5.
Improve the facial profile.
- 6.
Obtain normal overjet and interincisal guidance.
- 7.
Reduce the mandibular incisor protrusion.
Treatment alternatives
Surgical exposure and orthodontic traction could be a possible approach for management of the impacted maxillary right canine. However, there was not adequate space to move the canine into correct alignment and to increase the mesiodistal width of the lateral incisor. So, since the maxillary right first premolar was in a Class I relationship with the mandibular right canine, it would be necessary to distalize the maxillary posterior teeth or extract a tooth (premolar or molar). The maxillary right canine was dilacerated and impacted in an oblique position, and it would also be difficult to retract without root resorption.
We could visualize closure of the maxillary left first molar space. But it was not the choice of treatment because of the vertical and buccolingual bone defect. Thus, a dental implant was indicated.
A practical way to solve the problem of the missing mandibular teeth would be to open space to insert dental implants in the mandibular first molar areas. Nevertheless, the patient preferred to reduce the surgical procedures, the number of dental restorations, and costs. Hence, the closure of those spaces with protraction of the mandibular second molars and retraction of anterior teeth into the maxillary left first molar area was the choice of treatment.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


