This report describes the treatment of a 16-year-old girl with a severe transverse dental arch discrepancy resulting from a mildly constricted maxillary arch and an overexpanded mandibular arch. The patient had a Class I skeletal relationship, a high mandibular plane angle, a Class III molar relationship, bilateral posterior crossbites, and deviated midlines. A 3-dimensional digital setup was used to assist treatment planning. The digital setup allowed us to evaluate multiple treatment options before deciding on the most suitable one for the patient. The final treatment protocol consisted of extraction of upper second premolars and lower first molars due to enamel hypoplasia. Starting with the leveling and alignment stage of treatment, the maxillary archwires were expanded and the mandibular wires were constricted to correct the transverse discrepancy. An auxiliary expansion arch was used to achieve overcorrection. The active treatment period was 24 months. Proper overbite and overjet, facial balance, and good occlusion were achieved.
A posterior crossbite typically results from a constricted maxillary arch width. Maxillary expansion is a valid way to solve this problem. However, in a few patients, the problem lies in the mandible: ie, excessive mandibular width. Mandibular width is more difficult to alter, regardless of expansion or constriction. Surgical measures can be adopted at added risks and costs.
Diagnosis and etiology
The patient was a 16-year-old Chinese girl. Her chief complaints were “crowded teeth and difficulty eating.” After having been declined by other clinics her parents brought her to our department. Her medical and dental histories were unremarkable. The extraoral examination showed that she had a slightly convex profile. Her lips were competent at rest but had moderate hypermentalis activity ( Fig 1 ). There were no temporomandibular joint symptoms, and mandibular movements were normal. The clinical examination along with the photographs showed that the maxillary dental midline coincided with the facial midline, and the mandibular midline was shifted to the right side by 2 mm. Enamel hypoplasia was noted on all first molars, especially the mandibular ones. Generalized mild gingivitis associated with fair oral hygiene was noted, but probing depths were within the normal limits.
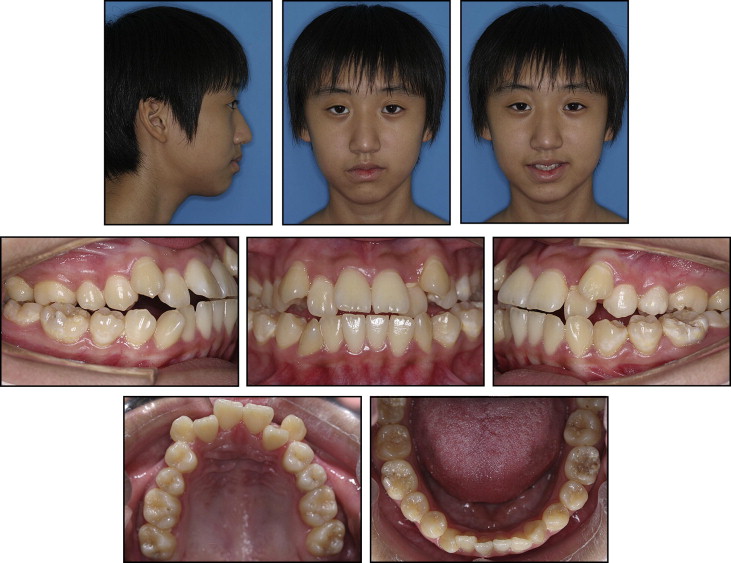
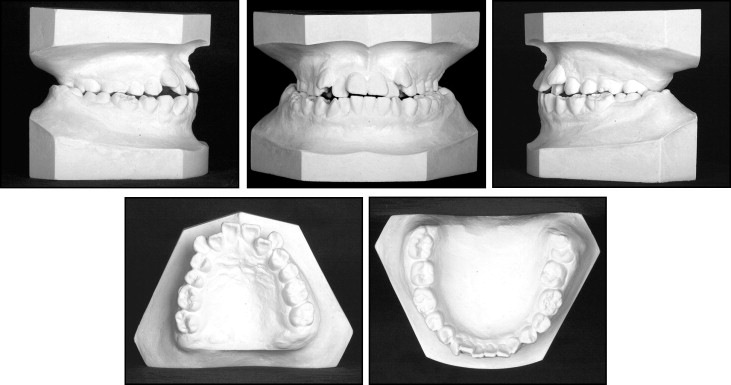
The dental casts showed Class III molar and canine relationships, and most of the posterior teeth were in crossbite with unstable occlusal contacts ( Fig 2 ). The maxillary arch was symmetrical and tapered in shape with 11 mm of crowding in the anterior region. The patient had a 1-mm overjet and a 1-mm open bite. The left lateral incisors were in crossbite as well. The mandibular arch was symmetrical and had a rounded form with 5 mm of crowding. Maxillary arch intercanine and intermolar widths were within normal limits, but the same measurements in the mandibular arch were much greater than the norms ( Table I ).
| Maxilla | Mandible | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 3-3 | 4-4 | 5-5 | 6-6 | 7-7 | 3-3 | 4-4 | 5-5 | 6-6 | 7-7 | 8-8 | |
| Pretreatment | 34.1 | 36.3 | 42.8 | 49.0 | 54.7 | 23.2 | 34.6 | 46.1 | 56.7 | 55.6 | 60.6 |
| Nonextraction | 35.4 | 42.8 | 49.9 | 55.0 | 60.7 | 25.3 | 36.4 | 44.1 | 52.6 | 55.8 | 58.8 |
| U5L4 | 34.1 | 41.9 | 48.6 | 54.6 | 25.5 | 35.0 | 43.4 | 50.1 | 55.0 | ||
| U5U6 | 34.3 | 41.6 | 48.8 | 54.9 | 25.6 | 34.8 | 41.6 | 50.4 | 55.6 | ||
| Posttreatment | 34.5 | 41.8 | 48.6 | 55.0 | 25.4 | 34.7 | 41.6 | 50.8 | 56.2 | ||
The panoramic radiograph showed no missing teeth, except for the maxillary third molars. Thin condyles were noticed on the panoramic radiograph. Although the patient had no temporomandibular joint symptoms, an additional examination was undertaken to ensure that there was no abnormal condylar resorption. Based on the findings from the cone-beam computed tomography examinations (3DX; Morita, Kyoto, Japan), we made a diagnosis of condylar hypoplasia ( Fig 3 ).

The cephalometric analysis showed a Class I skeletal relationship. The mandibular plane was high with a steep occlusal plane (MP-SN angle, 49.7°; SN-OP angle, 28.9°). The lower facial height ratio was slightly increased. Dentally, the maxillary and mandibular incisors were moderately protrusive relative to the alveolar base ( Table II ). The patient was diagnosed with a Class III malocclusion and a Class I skeletal pattern with a high mandibular plane angle.
| Measurement | Mean | SD | Initial | Final |
|---|---|---|---|---|
| SNA (°) | 82.8 | 4.0 | 75.8 | 77.1 |
| SNB (°) | 80.1 | 3.9 | 73.1 | 74.2 |
| ANB (°) | 2.7 | 2.0 | 2.7 | 2.9 |
| A-NFH (mm) | 0.0 | 3.7 | −7.7 | −5.8 |
| Pg-NFH (mm) | −5.7 | 3.8 | −20.9 | −20.1 |
| Wits (mm) | −1.1 | 2.9 | −6.7 | −2.8 |
| MP/SN (°) | 32.5 | 5.2 | 49.7 | 49.4 |
| MP/FH (°) | 31.1 | 5.6 | 43.4 | 43.2 |
| MP/PP (°) | 27.6 | 4.6 | 40.7 | 37.4 |
| SN/OP (°) | 16.1 | 5.0 | 28.9 | 20.6 |
| FH/OP (°) | 12.4 | 4.4 | 22.6 | 14.5 |
| U1-AP (mm) | 7.2 | 2.2 | 10.6 | 7.5 |
| L1-AP (mm) | 4.9 | 2.1 | 8.0 | 4.8 |
| U1/PP (°) | 115.8 | 5.7 | 121.3 | 111.4 |
| L1/MP (°) | 93.9 | 6.2 | 88.4 | 85.6 |
| U1/L1 (°) | 124.2 | 8.2 | 110.0 | 125.4 |
| Upper lip–E-line (mm) | −2.5 | 1.5 | −1.2 | −2.9 |
| Lower lip–E-line (mm) | 1.4 | 1.9 | 3.4 | 0.6 |
The lateral cervical vertebrae on the cephalometric radiograph showed that the patient had passed her growth peak, although some growth was expected during the treatment. The etiology of this malocclusion was unclear. A possible explanation was that the severe crowding in the maxillary arch along with the buccally displaced and inclined premolars and first molars in the mandibular arch caused the severe transverse discrepancy.
Treatment objectives
The treatment objectives were to correct the Class III malocclusion, correct the transverse discrepancy, alleviate the crowding, achieve proper dental inclination, correct the anterior open bite, and correct the midline deviation. The high mandibular plane should be at least maintained or even improved by attempting to produce counterclockwise rotation of the mandible to improve the profile.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


