Introduction
Posterior unilateral crossbite treatment is usually oriented to the maxilla. The aims of this retrospective investigation were (1) to study the maxillary arch morphology in patients with posterior unilateral crossbite and (2) to evaluate the possible association between the transverse maxillary arch morphology and the skeletal symmetry or asymmetry of the corresponding mandible.
Methods
Data from maxillary arch occlusograms and posteroanterior and panoramic radiograph tracings of the mandible were obtained for 94 patients with posterior unilateral crossbite and midline deviation. A multiple linear regression model was used to assess the association of transverse maxillary arch morphology with demographic and clinical characteristics. The prevalence of skeletal asymmetry was modeled by using a multiple logistic regression on transverse maxillary arch morphology, adjusted for the patients’ characteristics.
Results
Three maxillary arch morphologies were found at the crossbite side: symmetric, contracted, and expanded. The expanded crossbite sides were statistically associated with mandibular asymmetry.
Conclusions
Different transverse maxillary arch forms at the crossbite side were observed in our patients with posterior unilateral crossbite. This finding might be interpreted as a diagnostic and prognostic key for mandibular asymmetry, paving the way for new treatment directions.
Posterior unilateral crossbite is characterized by the lingual inversion of the normal transverse dental relationship. It must include at least 1 posterior tooth on 1 side and is often supported by a maxillary transverse contraction with respect to the mandible. This relatively frequent disharmony (8.7%-23.3%) is usually associated with a lateral shift of the mandible, mostly toward the crossbite side, when passing from rest or centric position to maximal intercuspal position (functional posterior unilateral crossbite, 67%-79%). Except for the more severe cases associated with congenital anomalies and craniofacial syndromes, posterior unilateral crossbite can be ascribed to skeletal, dental, and functional asymmetries, or to a combination of these factors.
Two fundamental issues led us to investigate how all of these components interact and contribute in the malocclusion. First, it is widely accepted that morphology is the principal key to diagnosis. Second, according to Enlow, growth of each facial region is linked to that of other structural counterparts. As a consequence, any alteration in some portion of the craniofacial complex produces an equal alteration in another part, aiming at a functional final balance. Imbalance results from differences in the quantity or the direction of growth between parts and counterparts.
Because of the importance of morphology, our first aim was to study the transverse maxillary arch form in patients with posterior unilateral crossbite and determine possible associations with other aspects of this malocclusion. Demographic and clinical characteristics, such as sex and age, type of malocclusion (symmetric or asymmetric), and crossbite extension (number of teeth involved), were investigated. Because the anteroposterior position of the first molars might affect asymmetric malocclusions, side-to-side maxillary molar sagittal differences were included in our study. In turn, the possible contribution of rotations to the anteroposterior molar position could not be neglected. When abnormal or perverted muscular forces tend to throw the crowns of the maxillary teeth forward, the mesiolingual cusps resist displacement so strongly that the molars rotate bodily around this tenacious portion of the crown. Such a malposition will produce an end-to-end contact with the mandibular teeth, as commonly shown by the high prevalence of mesiolingual rotations in Class II malocclusions. To prevent distortions when evaluating maxillary molar sagittal positions, dental rotations were registered also.
Second, following Enlow’s theory, we hypothesized that different transverse maxillary morphologies might be correlated to alterations of their counterparts, the mandibles. Thus, we tested the relationship between transverse maxillary arch forms in unilateral posterior crossbites and the corresponding mandibular skeleton. In particular, we explored whether the specific maxillary morphologies in the transverse plane were prevalent in patients with skeletal mandibular asymmetry.
Material and methods
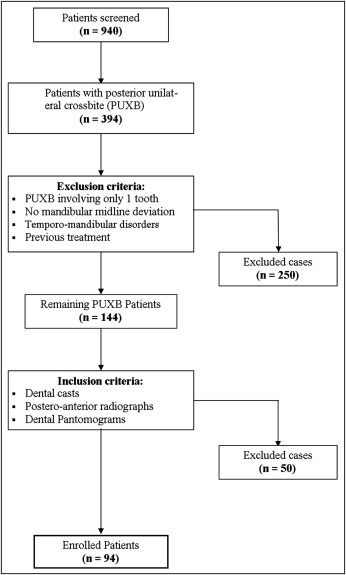
Of the 940 consecutive orthodontic patients who visited a private office from 1994 to 2008, those diagnosed with posterior unilateral crossbite were selected (n = 394). Inclusion criteria were the involvement of at least 2 adjacent posterior teeth and a mandibular midline deviation. Previously treated patients and those suffering from temporomandibular disorders were not included in this cross-sectional study. From the 144 remaining patients, those with dental casts, dental pantomograms, and posteroanterior radiographs of good quality, were included in our study ( Fig 1 ).
Maxillary dental arch morphology was investigated by means of dental casts. The skeletal symmetry of the mandible was diagnosed by using dental pantomograms and posteroanterior radiographs. All patients gave their consent for data publication.
The Angle malocclusions were diagnosed for the selected posterior unilateral crossbite patients. They were split into 2 groups based on the symmetry of the side-to-side molar relationship, independently from Angle Class I, Class II, or Class III malocclusion. More specifically, the malocclusion was classified as symmetric when the discrepancy between the right and left molar relationships was of the same severity (ie, 2.5 mm out of Class I relationship at both sides). For molar relationships of different extents (differences >0.5 mm; ie, 1 mm out of Class I on 1 side and 1.5 mm out of Class I on the other side), the subject was put in the asymmetric group. Those with Class II subdivisions (Class II on 1 side and Class I on the other side) were assigned to the asymmetric group.
Then the numbers of teeth involved in the crossbite were assessed. The teeth in the crossbite had to be at least 2, adjacent, and the most posterior on 1 side only of the arch to be included in our sample. Edge-to-edge teeth were not considered to be involved teeth.
The numbers of absent teeth in the whole arch—eg, first and second molars, respectively, in the deciduous and early permanent dentitions—were counted separately.
Occlusograms were obtained with the Kinast polygraph (Dr. H. Kinast, Austria). The 90° rotated dental casts were fixed through an arm to a plane, and, with a mirroring system, occlusal dental surfaces appeared on the diaphanoscope with a 1:1 enlargement ( Fig 2 ). The maxillary dental arch was traced in the transverse plane by 1 operator (P.S.). The dental variables identified on the occlusograms were the tips of the canine cusps, the premolar buccal cusps (or deciduous molar buccal cusps), and the mesiobuccal, mesiolingual, and distobuccal cusps of the first and second molars. These points were measured in relation to the palatal midline ( Fig 2 ), which was located according to 2 points along the palatal raphe: at the second palatal ruga and the most posterior point on the raphe. These points were chosen for their stability and reproducibility.
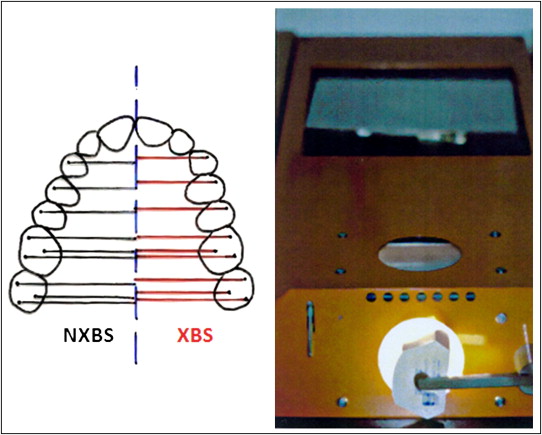
Each dental hemi-distance was measured at both the crossbite side and the noncrossbite side. All were registered independently from cross-extension. The average of all dental distances of the crossbite side was compared with that of the noncrossbite side by computing the differences between these 2 averages, here defined as the dental transverse difference. The value of the dental transverse difference, with reference to the crossbite side, could be negative (crossbite less than noncrossbite), positive (crossbite greater than noncrossbite), or neutral (crossbite and noncrossbite the same). Negative dental transverse difference values indicated that the average dental transverse distance at the crossbite side was closer to the midline rather than at the noncrossbite side. The associated clinical observations indicated a maxillary morphology contracted at the crossbite side. On the contrary, when the average transversal distance was increased at the crossbite side compared with that of the counterside (positive dental transverse difference values), the morphology of the crossbite side appeared expanded. For equal dental distances of the crossbite and noncrossbite sides from the midline, a neutral dental transverse difference was registered to indicate a symmetric maxillary arch. Hence, the dental transverse difference was used to describe different maxillary arch morphologies in the patients with posterior unilateral crossbite.
Maxillary arch occlusograms included evaluation of the sagittal position differences and rotations of the first molar. The position difference was calculated as the difference between the measurements of the anteroposterior distances from the geometric center of the molar’s mesial surface to the interincisal papillae at both the crossbite and the noncrossbite sides. Molar rotations were judged according to the method of Friel. The angle between the raphe and a line through the mesiobuccal and mesiopalatal cusps of maxillary first molars was measured; these ranged from 55° to 65° for the right side and from 52° to 62° for the left side.
Radiographs were taken by an experienced operator (F.F.) using the same radiographic devices (Orthopantomograph 10 and Orthoceph 10S; Siemens, Bensheim, Germany) in standard conditions.
To ensure adequate reproducibility of the vertical and angular measurements, special attention was given to position each patient’s head properly in the equipment during exposure, as advocated in the literature. Dental pantomograms were taken by centering the patient’s head in the head holder of the device with a central light aligned with the nose, and with the Frankfort horizontal plane parallel to the floor. The forehead touched an appropriate support to prevent technical errors from head positioning. A bite-block was held between the incisors. Precise instructions were followed also for the posteroanterior radiographs. The posteroanterior radiographs were taken with the cranial support in habitual occlusion. A wax bite was held to enhance the accuracy in the evaluation of asymmetry when dental interferences dictated a significant mandibular shift. Patients’ heads were positioned with the midsagittal plane perpendicular to the film plane. Auricular olives were inserted in the auditory meati to minimize errors caused by head rotation. Asymmetric external auditory meati were not inspected, but the auricular olives were not forced into the external auditory meati.
Cephalometric tracings on posteroanterior radiographs and dental pantomograms were made with a 0.5-mm pencil on acetate paper by 1 operator (F.F.).
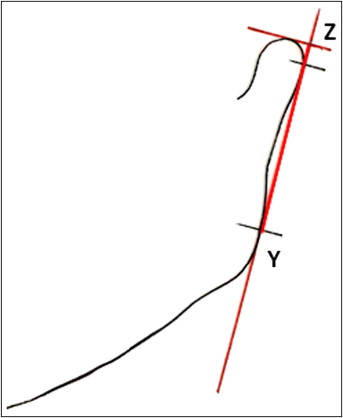
The study of the dental pantomograms involved ramus height measurement Z-Y, with Y defined as the most prominent low point of the posterior ramus edge, and Z as the intersection of the 2 tangents ( Fig 3 ). The first tangent was drawn to the posterior ramus passing through Y (ramus tangent); the second was drawn as the perpendicular to the ramus tangent passing through the top of the condyle (condylar tangent). Measurements of Z-Y at the crossbite and noncrossbite sides were translated to right and left values and used in the formula of Habets et al : ([right − left]/[right + left]) × 100% to assess diagnosis. According to Habets et al, an index value greater than 3% between the vertical sizes of the rami indicates potential ramus asymmetry, called skeletal asymmetry on dental pantomograms (SKEL DPT ) in our investigation. Mandibular body and total length measurements were not considered on the dental pantomograms because of the unreliability of menton.
On the posteroanterior radiographs, linear measurements of the mandibular body and ramus height were recorded at both the crossbite and noncrossbite sides.
Determinations on dental pantomograms and posteroanterior radiographs were performed once more for 30 subjects randomly selected by 2 researchers independently (F.F. and P.S.) to determine the repeatability of landmark identification and measurement techniques. The paired-samples t test was used to evaluate the difference between the first and second measurements. The Bland and Altman plot was used to assess the agreement of the measurements from the 2 researchers.
Demographic and clinical characteristics of the selected patients are shown in Table I .
| Characteristic | Value |
|---|---|
| Sex | |
| Female | 60 (63.8%) |
| Male | 34 (36.2%) |
| Age (y) | 8.61 (7.02, 9.88) |
| IT | |
| 2 teeth | 1 (1.1%) |
| 3 teeth | 11 (11.7%) |
| 4 teeth | 7 (7.4%) |
| 5 teeth | 75 (79.8%) |
| AT | |
| 0 teeth | 5 (5.3%) |
| 1 tooth | 66 (70.2%) |
| 2 teeth | 21 (22.3%) |
| 3 teeth | 1 (1.1%) |
| 4 teeth | 1 (1.1%) |
| Shift | |
| XBS | 86 (91.5%) |
| NXBS | 8 (8.5%) |
| Molar relationship | |
| Symmetric | 36 (38.3%) |
| Asymmetric | 58 (61.7%) |
| DTD | −0.55 (−1.36, 0.12) |
| Ramus DPT (Habets et al ) | 0.011 (0.000, 0.024) |
| Ramus PA (Habets et al ) | 0.008 (0.004, 0.013) |
| Body PA (Habets et al ) | 0.012 (0.006, 0.024) |
| 6SPd | 0.00 (−0.50, 1.00) |
| MR left side | 54 (50, 59) |
| MR right side | 53 (46, 57) |
The primary outcome variables were the dental transverse maxillary difference between the crossbite and noncrossbite sides and the potential skeletal ramus asymmetry, as detected with the formula of Habets et al on the dental pantomograms (SKEL DPT ).
A multiple linear regression model was used to assess the association of transverse maxillary arch morphology (dental transverse difference) with the patients’ characteristics: sex, age at the first visit, symmetry or asymmetry of malocclusion, sagittal molar position and rotation, and numbers of teeth involved in the crossbite, adjusting for the number of absent teeth as reported in Table II .
| Variable | Coefficient (95% CI) | P value |
|---|---|---|
| Sex (male) | −0.498 (−1.029, 0.034) | 0.066 |
| Age (y) | 0.004 (−0.118, 0.127) | 0.941 |
| Molar relationship (sym) | −0.102 (−0.616, 0.413) | 0.695 |
| 6SPd | −0.236 (−0.441, −0.032) | 0.024 † |
| IT | 0.438 (0.118, 0.758) | 0.008 † |
| MR left side | 0.017 (−0.020, 0.054) | 0.361 |
| MR right side | 0.001 (−0.034, 0.036) | 0.955 |
∗ Results were calculated with the use of a multiple linear regression on DTD, adjusted for absent teeth.
A multiple logistic regression model was used to assess the association of dental transverse difference with ramus asymmetry (SKEL DPT ), adjusting for the patients’ characteristics ( Table III ). For a more reliable analysis, exact inference methods were adopted to prevent assumptions about the null distribution. To simplify the interpretation of the results, age at the first visit was categorized into tertiles, and the number of teeth involved in the crossbite was split into 2 groups of 5 teeth and less than 5 teeth. The difference in anteroposterior molar position between the crossbite and the noncrossbite sides (first molar sagittal position difference) was categorized into 3 groups according to the sign (negative, zero, or positive). Molar rotations were registered for both sides.
| Variable | Not SKEL DPT (n = 78) n (%) | SKEL DPT (n = 16) n (%) | Odds ratio (95% CI) | P value |
|---|---|---|---|---|
| Sex | ||||
| Female | 52 (66.7) | 8 (50.0) | 1 | |
| Male | 26 (33.3) | 8 (50.0) | 4.36 (0.99, 26.5) | 0.052 |
| Age (y) | ||||
| <8 | 27 (34.6) | 7 (43.8) | 1 | |
| 8-10 | 32 (41.0) | 6 (37.5) | 0.63 (0.1, 3.66) | 0.805 |
| >10 | 19 (24.4) | 3 (18.8) | 0.90 (0.05, 2.66) | 0.999 |
| Molar relationship | ||||
| Symmetric | 31 (39.7) | 5 (31.2) | 1 | |
| Asymmetric | 47 (60.3) | 11 (68.8) | 1 (0.2, 4.64) | 0.999 |
| 6SPd | ||||
| <0 | 22 (28.2) | 3 (18.8) | 1 | |
| 0 | 21 (26.9) | 4 (25.0) | 1.84 (0.19, 21.35) | 0.853 |
| >0 | 35 (44.9) | 9 (56.2) | 1.95 (0.34, 16.43) | 0.656 |
| IT | ||||
| 5 | 17 (21.8) | 2 (12.5) | 1 | |
| <5 | 61 (78.2) | 14 (87.5) | 1.85 (0.24, 24.31) | 0.823 |
| DTD | ||||
| Contracted | 39 (50.0) | 5 (31.2) | 1.09 (0.17, 7.71) | 0.999 |
| Symmetric | 34 (43.6) | 4 (25.0) | 1 | |
| Expanded | 5 (6.4) | 7 (43.8) | 14.63 (2.04, 173.12) | 0.004 † |
∗ A multiple exact logistic regression was used including all covariates and stratified by absent teeth (values coded into 0, 1, and ≥2 strata).
The dental transverse difference threshold value () was used to categorize the maxillary morphologies into 3 classes: contracted (dental transverse difference, <−), symmetric (− ≤dental transverse difference ≤), and expanded (dental transverse difference, >). The threshold was chosen in a set of 1000 different values between 0.01 and 1 mm with an iterative procedure evaluating which value maximized the likelihood function of the multiple logistic regression model of SKEL DPT .
The secondary endpoint was the skeletal asymmetry found with the posteroanterior radiograph measurements for both the mandibular ramus and the body, called skeletal asymmetry on posteroanterior radiographs (SKEL PA ).
Because of the lack of recognized standards to diagnose mandibular asymmetry, we defined our outcome by exploring the relationship between the dental pantomogram and the posteroanterior radiograph measurements of the rami. To this aim, a simple logistic model of the class label for ramus (a)symmetry diagnosed on dental pantomograms was adopted, including the index of Habets et al calculated on the posteroanterior radiograph measurements of the ramus as a predictor. The area under the receiver operating characteristic curve was used to evaluate the discriminant ability of the model. This model was subsequently used to calibrate ramus and body measurements on the posteroanterior radiographs to detect skeletal asymmetry (SKEL PA ).
Results of the exact multiple logistic-regression model were used to estimate the independent effect of maxillary dental transverse differences on the prevalence of SKEL PA , adjusting for the patients’ characteristics ( Table IV ). Discrete data are presented as frequencies and percentages, and continuous variables as medians and interquartile ranges.


