Introduction
The purposes of this study were to compare the buccolingual inclinations of the posterior teeth in skeletal Class III patients with and without facial asymmetry with those of skeletal Class I patients and to investigate their relationships with sagittal and transverse skeletal discrepancies.
Methods
Sixty-three skeletal Class III adult patients were divided into 2 groups according to the degree of menton deviation: a symmetry group with deviation less than 2 mm (n = 30), and an asymmetry group with deviation greater than 4 mm (n = 33). The control group comprised 25 skeletal Class I patients. The buccolingual inclinations of the posterior teeth measured on cone-beam computed tomography images were compared among the 3 groups, and regression analysis was performed to investigate the relationships between the inclinations and the sagittal and transverse skeletal discrepancies.
Results
The symmetry group showed greater buccal inclinations of the maxillary posterior teeth and lingual inclinations of the mandibular second molars than did the control, and this was correlated with the ANB angles. The deviated sides in the asymmetry group showed the greatest transverse dental compensation, which was correlated with menton deviation, whereas the nondeviated sides showed no significant transverse dental compensation.
Conclusions
Transverse dental compensation is closely related to sagittal and transverse skeletal discrepancy in skeletal Class III patients.
Highlights
- •
We compared skeletal Class III and Class I patients.
- •
Class III patients had more buccal inclination of the maxillary posterior teeth.
- •
Class III patients had more lingual inclination of the mandibular second molars.
- •
Deviated side in Class III patients with asymmetry showed transverse dental compensation.
- •
Nondeviated side showed no significant transverse dental compensation.
- •
Transverse dental compensation was closely related to skeletal discrepancies.
The buccolingual inclinations of the posterior teeth are critical for establishing an ideal occlusion. It is a fundamental factor when determining the prescription of a straight-wire appliance. In this regard, the American Board of Orthodontics Objective Grading System includes an evaluation criterion for buccolingual inclination of the posterior teeth.
Traditionally, buccolingual inclination of the posterior teeth has been determined using either dental casts or posteroanterior cephalograms, but both methods have inherent limitations. The inclinations using the tangent point of the buccal crown contour and the occlusal plane on dental casts rarely coincide with the inclination of the roots. A posteroanterior cephalogram may show the inclination of the roots, but superimposition of the anatomic structures and the teeth decreases the reliability of this method. Recently, cone-beam computed tomography (CBCT) has enabled evaluation of the mesiodistal angulation and the buccolingual inclination of the whole tooth, including crown and roots.
Transverse discrepancy is a common problem and more frequently found in skeletal Class III patients. This is not only because some skeletal Class III patients have an underdeveloped maxilla and an overdeveloped mandible with a low tongue posture, resulting in an absolute transverse discrepancy, but also because the relative forward position of the mandible leads to a relative transverse discrepancy. Labiolingual inclinations of the maxillary and mandibular anterior teeth are a major dental compensation for a sagittal skeletal discrepancy in skeletal Class III patients, so that posterior teeth also show a transverse dental compensation in patients with a transverse skeletal discrepancy. The pattern of transverse dental compensation is more complicated when there is facial asymmetry, which is found in nearly half of skeletal Class III patients. Understanding the mechanism of transverse dental compensation is crucial when planning appropriate camouflage and presurgical orthodontic treatment for such patients, because whether to expand or constrict the maxillary or mandibular arch largely depends on the buccolingual inclination of the posterior teeth and the preexisting transverse dental compensation.
Several studies have investigated transverse dental compensation in skeletal Class III patients with facial asymmetry using computed tomographic images. However, these studies have either lacked a skeletal Class I control group or a skeletal Class III group without facial asymmetry. Transverse dental compensation is affected by both sagittal and transverse skeletal relationships, so it is necessary to compare a skeletal Class I group with skeletal Class III groups with and without facial asymmetry to show the mechanism fully. Moreover, previous studies have focused only on the first molars, when transverse dental compensation affects all posterior teeth, and the pattern of compensation may differ from tooth to tooth.
The aims of this study were to compare transverse dental compensation patterns of the posterior teeth between skeletal Class III patients with and without facial asymmetry and skeletal Class I patients and to investigate their relationships with sagittal and transverse skeletal discrepancies.
Material and methods
This study was approved by the institutional review board of Gangnam Severance Dental Hospital (No. 3-2015-0091) in Seoul, Korea. The CBCT scans of patients who visited its Department of Orthodontics from 2011 through 2014 were screened to select the experimental and control groups.
Eighty-three skeletal Class III subjects who satisfied the following criteria were included in the experimental group: (1) age over 18 years and without previous orthodontic treatment, (2) ANB angle less than 0°, (3) fully erupted permanent premolars and molars without ectopic eruption or apparent crowding, (4) no missing or extracted teeth, (5) no crowns or cuspal restorations of the posterior teeth, (6) no systemic disease, and (7) no cleft lip or palate or temporomandibular joint disease. The subjects were divided into groups according to the amount of menton (Me) deviation from the midsagittal plane measured in 3-dimensional (3D) CBCT images: (1) skeletal Class III, symmetry, with Me deviation less than 2 mm (group S); and (2) skeletal Class III, asymmetry, with Me deviation greater than 4 mm (group AS). Twenty borderline cases of Me deviation between 2 and 4 mm were excluded from the study. Finally, 30 patients were enrolled in group S (17 men, 13 women) and 33 patients in group AS (15 men, 18 women).
The control group (group I) comprised 25 patients (11 men, 14 women) selected by the following criteria: (1) ANB between 1° and 4° and Me deviation less than 2 mm, (2) anterior crowding less than 4 mm, (3) no buccal or lingual crossbite of posterior teeth, and (4) other criteria the same as above. Table I summarizes the patients’ characteristics.
| Skeletal Class I (n = 25) (mean ± SD) | Skeletal Class III, symmetry (n = 30) (mean ± SD) | Skeletal Class III, asymmetry (n = 33) (mean ± SD) | Multiple comparison | |
|---|---|---|---|---|
| Age (y) | 22.7 ± 5.31 | 22.9 ± 4.16 | 21.7 ± 3.77 | |
| ANB (°) | 2.6 ± 0.89 | −1.9 ± 1.53 | −1.7 ± 1.60 | S = AS < I |
| Me deviation (mm) | 1.2 ± 0.64 | 1.0 ± 0.51 | 8.4 ± 3.09 | S = I < AS |
The CBCT scans (PaX-Zenith 3D; Vatech, Gyeonggi-Do, Korea) were performed under the following conditions: 120 kV, 10 mA, and voxel size of 0.3 mm. The scanned images were saved as digital imaging and communication in medicine (DICOM) files and reconstructed into 3D images using the OnDemand 3D software program (version 1.0; Cybermed, Seoul, Korea). The reconstructed 3D images were reoriented using the Frankfort horizontal plane as horizontal and midsagittal planes passing through nasion and basion and perpendicular to the Frankfort horizontal plane. Landmarks and reference planes are defined in Table II and Figure 1 .
| Definition | |
|---|---|
| Landmark | |
| N (nasion) | Middle point between frontal bone and nasal bone |
| Ba (basion) | Most anterior point of foramen magnum |
| Or (orbitale) | Lowest point of lower margin of orbit |
| Me (menton) | Most inferior point on symphysis of mandible |
| Po (porion) | Most superior point of external auditory meatus |
| Reference planes | |
| FH (Frankfort horizontal) plane | Plane passing through right porion, left porion, and midpoint of left and right orbitale |
| Midsagittal plane | Plane perpendicular to FH plane, passing through nasion and basion |
| Angular measurements | |
| Long-axis plane | Plane perpendicular to the midsagittal plane and passing through the mesial cusp and mesial root apex in molars and the cusp tip and root apex in premolars |
| Maxilla | |
| Long axis, multirooted premolar and molar | Line connecting the groove between the buccal and palatal cusps and the furcation of the roots |
| Long axis, single-rooted premolar | Line connecting the groove between the buccal and palatal cusps and the root apex |
| Reference line | FH plane in the long-axis plane shown as a line |
| Mandible | |
| Long axis, premolar and molar | Line connecting the groove between the buccal and lingual cusps and the root apex |
| Reference line | Tangent line to the inferior border of the mandible |
Me deviation was measured as the distance between Me and the midsagittal plane. Since the amount of Me deviation was not zero in all patients, the deviated side was defined as the side toward which the Me was deviated in relation to the midsagittal plane, and the other side was defined as the nondeviated side.
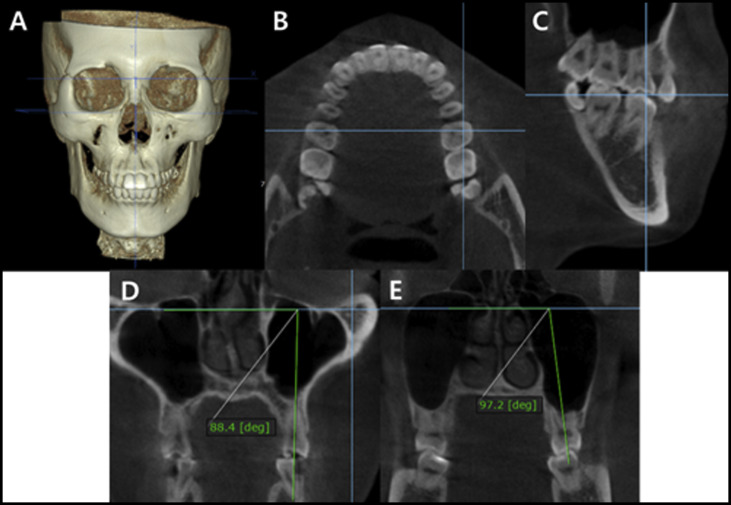
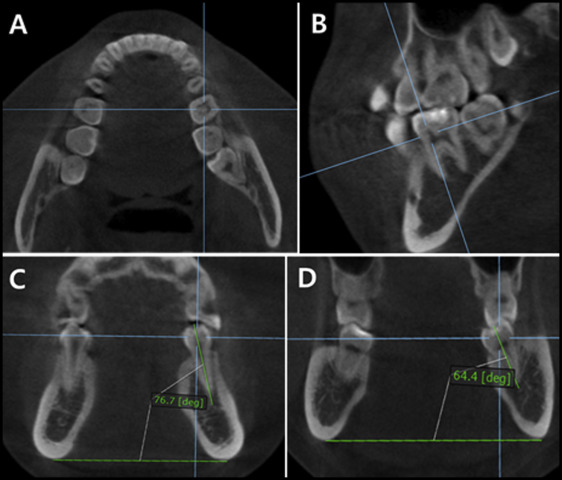
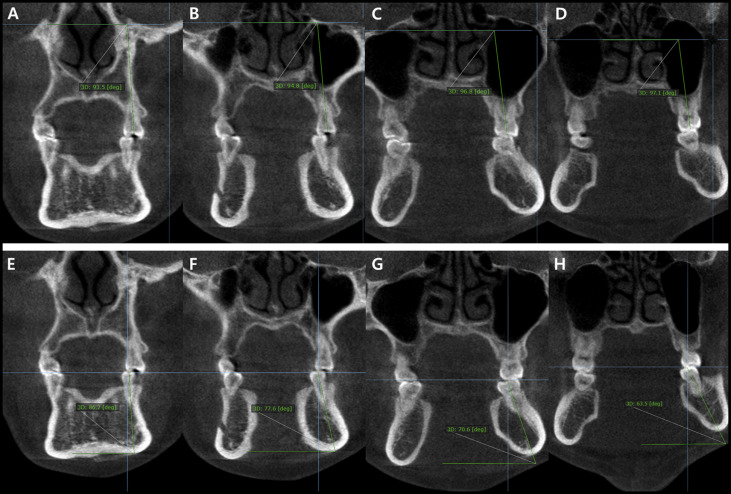
To measure the buccolingual inclination of the posterior teeth, long-axis planes were defined as planes perpendicular to the midsagittal plane and passing through the mesial cusp and mesial root apex of the molars, and the cusp tip and root apex of the premolars. Buccolingual inclinations were measured on the long-axis planes as an angle between the long axis of each tooth and the Frankfort horizontal plane for the maxillary teeth and a line connecting the mandibular inferior borders on both sides for the mandibular teeth ( Table II ; Figs 2 and 3 ). Figure 4 is representative CBCT images at the long-axis planes of a patient in group I, showing the buccolingual inclinations of the posterior teeth.
Statistical analysis
All buccolingual inclinations on the CBCT images were remeasured after a 2-week interval in 20 patients selected at random by 2 authors (J.A. and S.J.K.). The repeated measurements done by these observers were used to calculate the intraclass correlation coefficient (ICC) for intraobserver reliability, and their first and second measurements were compared for interobserver reliability. Paired t tests were used to examine the differences in inclination between the deviated sides and nondeviated sides in each group. One-way analysis of variance (ANOVA) and post hoc Bonferroni tests were used to compare the buccolingual inclination of the posterior teeth between Group I, S, deviated side of AS and non-deviated side of AS. In groups I and S, linear regression analysis was performed to detect the impact of the sagittal skeletal discrepancy (ANB angle) on the buccolingual inclination of the posterior teeth. In groups S and AS, linear regression analysis was carried out to detect the influence of the transverse skeletal discrepancy (Me deviation) on the buccolingual inclination of the posterior teeth. All statistical analyses were performed with Statistical Package for the Social Sciences software (version 20; IBM, Armonk, NY). A P value less than 0.05 was considered to be statistically significant.
Results
The ICC values ranged from 0.931 to 0.948 for intraobserver reliability and from 0.908 to 0.925 for interobserver reliability, indicating excellent reproducibility of the measurements. There was no significant difference in buccolingual inclinations between the deviated and nondeviated sides in groups I and S ( P >0.05). In group AS, the maxillary teeth were more buccally inclined and the mandibular teeth were more lingually inclined on the deviated sides than on the nondeviated sides ( P <0.001; Table III ). Therefore, the buccolingual inclination values for both sides were combined in groups I and S, and group AS was further divided into deviated sides (group D) and nondeviated sides (group ND) for subsequent group comparisons.
| Skeletal Class I (n = 25) | Skeletal Class III, symmetry (n = 30) | Skeletal Class III, asymmetry (n = 33) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Deviated side (mean ± SD) | Nondeviated side (mean ± SD) | P value | Deviated side (mean ± SD) | Nondeviated side (mean ± SD) | P value | Deviated side (mean ± SD) | Nondeviated side (mean ± SD) | P value | |
| Inclination of maxillary teeth (°) | |||||||||
| 4 | 88.4 ± 5.18 | 86.7 ± 4.77 | 0.069 | 90.7 ± 6.51 | 90.8 ± 4.94 | 0.953 | 94.2 ± 5.60 | 87.0 ± 5.57 | <0.001 ∗ |
| 5 | 91.0 ± 4.44 | 90.5 ± 4.71 | 0.638 | 94.1 ± 5.90 | 95.0 ± 5.72 | 0.075 | 99.3 ± 5.28 | 89.6 ± 5.29 | <0.001 ∗ |
| 6 | 93.6 ± 4.91 | 91.3 ± 4.62 | 0.053 | 97.0 ± 4.21 | 97.4 ± 3.75 | 0.450 | 101.0 ± 4.87 | 90.4 ± 6.04 | <0.001 ∗ |
| 7 | 99.8 ± 4.11 | 97.9 ± 5.60 | 0.093 | 102.4 ± 5.49 | 103.3 ± 5.74 | 0.308 | 109.3 ± 7.01 | 100.3 ± 8.74 | <0.001 ∗ |
| Inclination of mandibular teeth (°) | |||||||||
| 4 | 90.2 ± 4.09 | 91.8 ± 6.43 | 0.176 | 88.7 ± 4.90 | 88.2 ± 4.02 | 0.655 | 81.9 ± 6.76 | 90.5 ± 3.51 | <0.001 ∗ |
| 5 | 84.0 ± 5.59 | 83.3 ± 5.26 | 0.639 | 82.4 ± 6.01 | 83.1 ± 4.40 | 0.540 | 76.6 ± 7.56 | 85.2 ± 4.67 | <0.001 ∗ |
| 6 | 76.7 ± 6.24 | 78.8 ± 4.87 | 0.135 | 77.5 ± 4.46 | 78.4 ± 4.44 | 0.363 | 73.2 ± 6.19 | 82.7 ± 6.10 | <0.001 ∗ |
| 7 | 76.9 ± 5.75 | 77.1 ± 6.20 | 0.855 | 71.4 ± 7.32 | 72.2 ± 6.64 | 0.560 | 65.8 ± 8.01 | 76.9 ± 7.76 | <0.001 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


