Introduction
The aim of this prospective clinical study was to evaluate the dentoalveolar effects of a palatal miniscrew-supported molar distalization appliance using a 3-dimensional reverse engineering method.
Methods
This study sample comprised 21 patients at an average age of 13.6 years with a bilateral Class II molar relationship. Distalization was performed using skeletal anchorage. Dental casts were obtained just before treatment and after appliance removal, and they were scanned with a 3-dimensional dental scanner. The digital dental cast images were aligned. Four points and 2 lines were determined on each tooth, and the correlations between tooth movements and the linear and angular changes were analyzed 3 dimensionally.
Results
In the sagittal direction, the first molars showed a mean linear movement of 4.10 ± 1.57 mm, with distal tipping of 11.02°; the central incisors showed a mean distal movement of 0.95 ± 0.40 mm, with retroclination of 1.59 ± 0.59°. In the vertical direction, only the first molars showed intrusion, with a mean value of –0.59 ± 0.50 mm. Rotation of the first molars was 4.92° ± 3.09°. The second molars had the greatest rotation. The highest correlation among tooth movements was found between the first and second molars.
Conclusions
Through support from the anterior palatal region, the maxillary first molars were distalized without anchorage loss. Furthermore, movement was observed in all 3 planes of space with reduction from the posterior to the anterior in the maxillary arch.
Highlights
- •
Palatal miniscrew-supported molar distalization was studied with 3D reverse engineering.
- •
Maxillary teeth were moved distally without anchorage loss.
- •
Movement was observed in 3 planes of space.
Maxillary molar distalization is a nonextraction treatment modality to gain space in the maxillary arch. The indication for maxillary molar distalization is a Class II dental relationship (due to mesial migration of maxillary posterior teeth) or a minor skeletal Class II relationship and mild or no mandibular tooth size–arch length discrepancy. The traditional method used for maxillary molar distalization is headgear (extraoral anchorage). However, headgear has some disadvantages; it is esthetically unacceptable and needs patient compliance. These disadvantages led to the development of intraoral distalization methods that do not require patient cooperation: eg, magnets, nickel-titanium open-coil springs, pendulum appliance, Keles slider appliance, distal jet appliance, and several other methods. The common and unwanted side effect of these noncompliance methods is the mesial drift of the premolars and the incisors: ie, anchorage loss. To prevent anchorage loss, intraoral distalization methods take support from the skeletal structures with the help of temporary anchorage devices such as endosseous implants, miniplates, and miniscrews. Implants and miniplates have some disadvantages such as high costs and the need for additional surgery for placement and removal. Miniscrews, on the other hand, are preferred because they are cheaper and less invasive than other methods. Additionally, they can be easily placed in several skeletal regions. The anterior palate is considered to be a safe region for miniscrew insertion because it is far from the tooth roots and important anatomic structures. Another advantage of palatal anchored distalization mechanics is that there is no need to use full fixed appliances during the distalization period. Many authors have examined the effects of intraoral distalization performed with support from the miniscrews placed in this region. However, the tooth movements were generally analyzed 2 dimensionally on cephalometric radiographs and dental cast photocopies in these studies. The recently emerged prominent opinion for the 3-dimensional (3D) analysis of tooth movements is the reverse engineering method. Until today, this method was used to analyze facial soft tissues, and skeletal and dental changes. Few studies have analyzed the dentoalveolar changes after molar distalization with digital casts. In this study, we aimed to evaluate how the maxillary teeth move in space with advanced reverse engineering software 3 dimensionally after maxillary first molar distalization through direct support from the miniscrews placed in the anterior palatal region.
Material and methods
Ethical approval for this prospective clinical study was obtained from the Ethical Committee of Gülhane Military Medical Academy in Ankara, Turkey. The patients signed consent forms before the study. The study was conducted with 21 subjects with an average age of 13.6 years, who were referred to the Department of Orthodontics of Gülhane Military Medical Academy for treatment. The study group consisted of 9 girls and 12 boys, and the mean age varied between 12.3 and 15.3 years. The subjects had skeletal Class I or mild Class II relationships (ANB, 2°-5°), with a normal facial vertical growth pattern, bilateral Class II molar relationship with moderate crowding (≤5 mm), fully erupted maxillary second molars and premolars, and mild or no crowding in the mandibular arch (≤3 mm). No orthodontic treatment was performed in the mandibular arch before or during the distalization period.
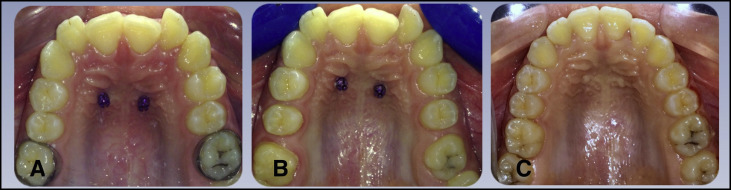
Two miniscrews, 1.7 mm in diameter and 8 mm in length (Forestadent, Pforzheim, Germany), were placed in the anterior palatal region corresponding to 6 mm posterior to the incisive papilla and 2 mm lateral to the sutura palatina media using the self-drilling method. A hyrax screw (Forestadent) was placed parallel to the occlusal plane by rotating it 90° so that it could open in the sagittal direction; hyrax arms were welded to the molar bands and abutments using a laser welding device (Tornado SL 75; Siro Lasertec, Pforzheim, Germany). One week after the placement of the miniscrews, the initial (T0) dental casts were obtained and the appliance was adapted; then the distalization period began ( Fig 1 ). The screw was activated by 0.2 mm every 5 days by the patient, and distalization was controlled every 4 weeks. Distalization was continued until a super-Class I molar relationship was achieved. At the end of distalization, the appliance was removed, the dental casts were taken (T1), the appliance was recemented for anchorage, and the treatment was continued ( Fig 2 ).

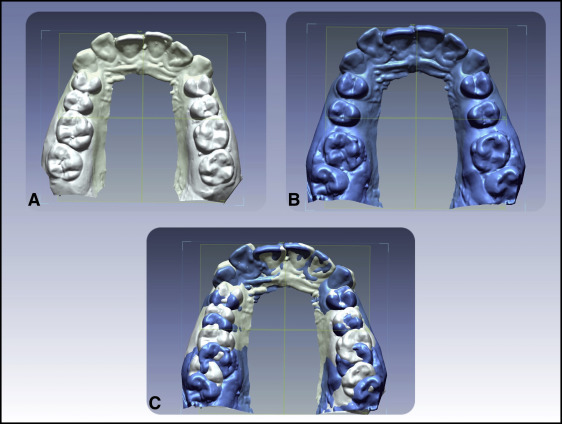
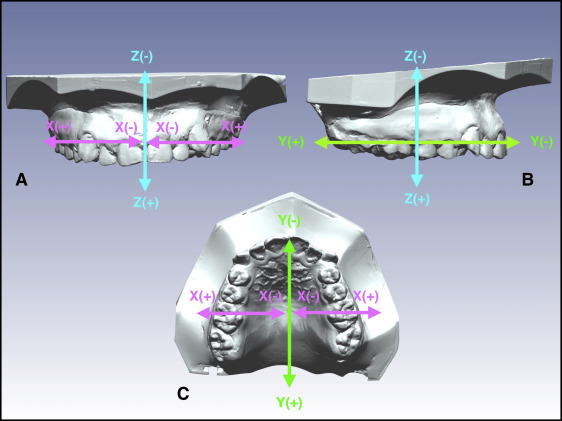
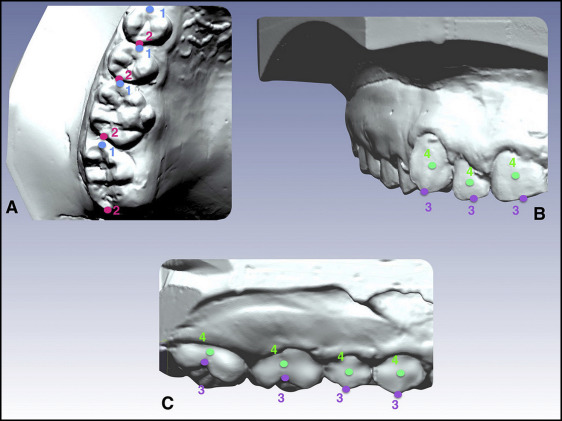
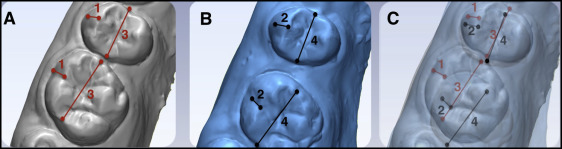
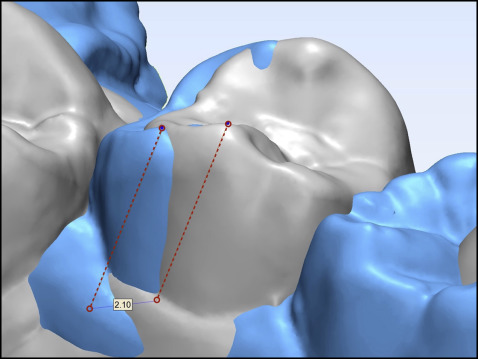
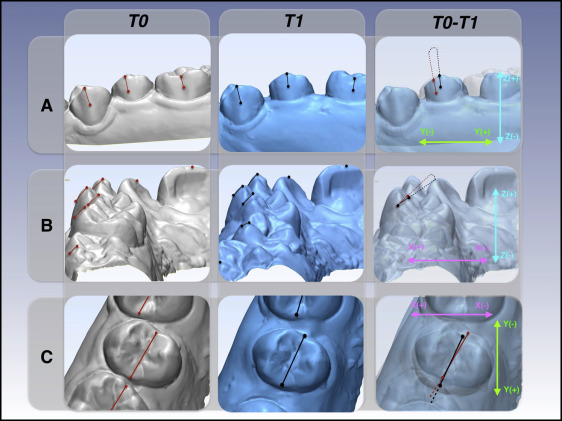
The dental casts from T0 and T1 were scanned with an optical dental scanner (Activity 850; Smart Optics, Bochum, Germany); the scans were converted into digital data, and the data were imported into reverse engineering software (Rapidform; INUS Technology, Seoul, South Korea) for the alignment phase. The T0 and T1 digital models of the same subject were aligned with the best fit (surface-to-surface matching) method ( Fig 3 ). The alignment procedure was performed on stable anatomic reference points such as the palatal rugae with limited manual process selection and deselection of this area. In this study, a standardized coordinate system was defined on the occlusal plane at T0 for all subjects ( Fig 4 ). Aligned digital models were imported to 3-matic Research software (Materialise, Haasrode, Belgium) for linear and angular measurements. Reference points and lines on each tooth in every model were determined by the same investigator (G.S.D.) ( Figs 5 and 6 ). The reference points and lines on the T0 and T1 models were transported into the aligned model (T0-T1). The distance between reference points was measured on the aligned models linearly in millimeters ( Fig 7 ) in the x, y, and z axes ( Fig 6 ). Similarly, the angles between reference lines were measured in degrees, and tipping, inclination, and rotation values were obtained ( Fig 8 ).
Statistical analysis
All statistical analyses and descriptive calculations were made using SPSS for Windows software (version 20.0; SPSS, Armonk, NY). The means, standard deviations, and minimum and maximum values of the linear and angular changes in the x, y, and z planes were calculated for all teeth. The total amount of linear movement ( D ) was calculated using the Euclidian distance formula.
The correlations among total linear movement amounts among the different teeth were evaluated using the Spearman rank correlation (r: positive linear correlation if r > 0; negative linear correlation if r < 0). The correlation was considered very weak if the coefficient was 0 to ≤0.25; weak, 0.26 to ≤0.49; moderate, 0.50 to ≤0.69; strong, 0.70 to ≤0.89; and very strong, 0.90 to ≤1.00. For evaluation of the methodologic errors, 15 patients were randomly selected from the 21 patients. Pretreatment and posttreatment measurements were repeated after 1 month by the same investigator, and intraobserver reliability was calculated using intraclass correlation coefficients for every measurement.
Results
Intraobserver reliability values (intraclass correlation coefficients) varied from 0.81 to 0.96 for all measurements. The average monthly distalization rate was 1.02 mm, and the mean duration of distalization was 5.30 ± 1.46 months (minimum, 3.9 months; maximum, 7.20 months). The survival rate of the paramedian miniscrews in our study was high; no miniscrew failure was observed. The amounts of the total movement and the linear movements in the transversal (x), sagittal (y), and vertical (z) planes for all teeth are presented in Table I .
| Tooth number | Distance (mm) | x-axis (mm) | y-axis (mm) | z-axis (mm) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | Min | Max | Mean | SD | Min | Max | Mean | SD | Min | Max | Mean | SD | |
| 1 | 0.27 | 1.67 | 0.95 | 0.40 | 0.01 | 0.87 | 0.34 | 0.21 | 0.01 | 1.62 | 0.59 | 0.37 | 0.02 | 1.13 | 0.38 | 0.32 |
| 2 | 0.01 | 1.98 | 0.91 | 0.47 | 0.04 | 1.10 | 0.49 | 0.28 | 0.03 | 1.93 | 0.64 | 0.45 | 0.05 | 1.43 | 0.46 | 0.32 |
| 3 | 0.65 | 3.50 | 2.00 | 0.72 | 0.23 | 1.84 | 0.77 | 0.39 | 0.05 | 2.74 | 0.93 | 0.63 | 0.44 | 5.20 | 1.44 | 0.80 |
| 4 | 0.75 | 4.13 | 1.99 | 1.02 | −0.02 | −1.45 | −0.46 | 0.36 | 0.35 | 3.95 | 1.61 | 0.94 | 0.01 | 1.63 | 0.70 | 0.40 |
| 5 | 1.20 | 4.96 | 2.79 | 1.05 | −0.10 | −1.12 | −0.51 | 0.28 | 1.19 | 5.37 | 2.90 | 1.08 | 0.08 | 1.28 | 0.52 | 0.30 |
| 6 | 2.13 | 7.69 | 4.67 | 1.32 | −0.03 | −1.86 | −0.69 | 0.44 | 0.86 | 6.98 | 4.10 | 1.57 | −0.01 | −2.30 | −0.59 | 0.50 |
| 7 | 1.34 | 7.81 | 3.77 | 1.33 | 0.21 | 2.26 | 1.16 | 0.55 | 1.15 | 6.54 | 3.30 | 1.25 | 0.05 | 4.15 | 1.03 | 0.76 |
When the amounts of total linear movement in all 3 planes were evaluated, the movement of the maxillary first molars was 4.67 ± 1.32 mm. These changes were 2.79 ± 1.05 mm for the second premolars and 3.77 ± 1.33 mm for the second molars. The lowest total movement was observed in the lateral incisors as 0.91 ± 0.47 mm.
The linear movement (y-axis) of the first molars was 4.10 ± 1.57 mm in the sagittal direction. The mean distal movement of the second premolars was 2.90 ± 1.08 mm. The lowest distal movement amount, which decreased toward the anterior teeth, was observed for the central incisors as 0.59 ± 0.37 mm. The distal movement of the second molars was 3.30 ± 1.25 mm.
For angular movements (yz-axis), the amounts of mean distal tipping were 11.02° ± 5.32° for the first molars and 6.21° ± 3.49° for the second premolars in the sagittal direction. The mean retroclination amount of the central incisors was 1.59° ± 0.91° ( Table II ).


