The prevention of plaque-induced diseases
Publisher Summary
This chapter discusses the ways to prevent plaque-induced diseases. Good dental health is usual in primitive societies where a fibrous and abrasive low-sugar diet provides for vigorous mastication, increased salivary flow, and self-cleansing and stimulation of the periodontal tissues. In contrast, the majority of people in modern industrialized societies consume a soft sugar-rich diet that provides for extensive bacterial fermentation leading to caries; as a result of under use, it also causes atrophy of the periodontium, which may lead to periodontal disease. These dietary associations are reinforced by epidemiological studies in developing countries, which show that an increase in the sugar content and degree of refinement of the diet is associated with a marked increase in the incidence of plaque-induced diseases. Thus, in Westernized societies, only a few individuals retain a complete and healthy dentition throughout their life, and methods of preventing dental disease become increasingly important. These are divided into a number of different categories, and include dietary control, plaque removal, treatment of the enamel surface, and various antibacterial measures. Effective prophylaxis is usually only obtained by a combination of several of these methods.
As mentioned earlier, good dental health is usual in primitive societies where a fibrous and abrasive low-sugar diet provides for vigorous mastication, increased salivary flow, self-cleansing and stimulation of the periodontal tissues. In contrast the majority of people in modern industrialized societies consume a soft sugar-rich diet which provides for extensive bacterial fermentation leading to caries; as a result of under use it also causes atrophy of the periodontium and this may lead to periodontal disease. These dietary associations are reinforced by epidemiological studies in developing countries which show that an increase in the sugar content and degree of refinement of the diet is associated with a marked increase in the incidence of plaque-induced diseases (Table 36.1). Thus in Westernized societies only a few individuals retain a complete and healthy dentition throughout their life and methods of preventing dental disease become increasingly important. These can be divided into a number of different categories and include dietary control, plaque removal, treatment of the enamel surface and various antibacterial measures. Effective prophylaxis is usually only obtained by a combination of several of these methods.
Table 36.1
The rapid increase in caries in developing countries. Average number of decayed, missing and filled teeth (DMFT) per child age 12
| 1950–1960 | 1970–79 | |
| Kenya | 0·1 | 1·7 |
| Uganda | 0·4 | 1·5 |
| Ethiopia | 0·2 | 1·6 |
| Iraq | 0·7 | 3·5 |
| Thailand | 0·7 | 4·5 |
| Vietnam | 2·0 | 6·3 |
| Polynesia | Approx. 0 | 8·0 |
| Industrialized countries (for comparison), children aged 13–14: | ||
| Sydney, Australia | 6·7 | |
| Canterbury, New Zealand | 10·7 | |
| Trondelag, Norway | 12·6 | |
| Hanover, Germany | 8·8 | |
| Yamakashi, Japan | 7·5 | |
| Bristol, England | 9·5 | |
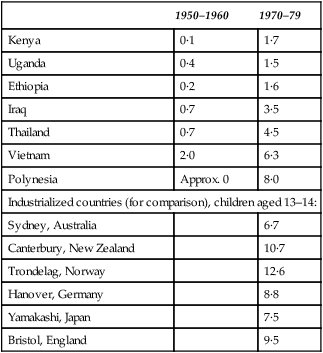
After Barmes (1977) Journal of Clinical Periodontology, 4, 80, and Andlaw et al. (1982) Caries Research, 16, 257
Dietary control
1. Dietary carbohydrates cause the pH at the tooth surface to fall below the critical pH for enamel dissolution.
2. Artificial carious lesions in enamel produced by acid-gels in vitro are indistinguishable from natural lesions.
3. Germ-free rats do not develop caries unless they are infected with bacteria from an animal with caries and are also fed a carbohydrate-rich diet.
4. Animals fed a cariogenic carbohydrate diet by mouth develop caries; those fed the same diet by stomach intubation do not.
5. The proportion of acid-forming bacteria in plaque samples from caries-active individuals is greater than in samples from caries-inactive individuals (Table 36.2). This ratio of acidogenic to total plaque organisms is significantly increased by supplementing the diet with sucrose.
Table 36.2
The ratio of acidogenic to total organisms in plaque samples from individuals with different caries histories
| Group | Mean ± standard deviation |
| Children | |
| Caries-free | 0·35 ± 0·01 |
| Caries-prone | 0·63 ± 0·01 |
| Students | |
| Caries-free | 0·42 ± 0·04 |
| Caries-prone: | |
| no recent lesions | 0·39 ± 0·07 |
| recent lesions | 0·59 ± 0·05 |
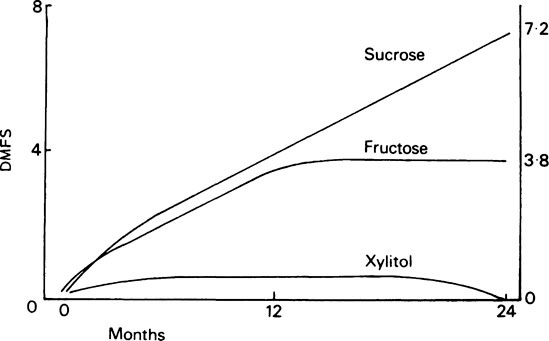
Observations at Hopewood House (1952–1956), a children’s home in Australia which maintained a nutritionally adequate but mainly vegetarian diet in which refined carbohydrates and sucrose were excluded, showed that the children had a low DMFT index which was not related to fluoride nor to good oral hygiene. When the children left the home at age 12–13 and were no longer under dietary control, their caries experience rapidly increased to match that of other children from state schools. A 2-year study at Turku Dental School, Finland, in 1976, in which caries-prone subjects totally replaced the sucrose in their diets with xylitol showed that this eliminated further caries progression when compared to a control group given sucrose- or fructose-containing diets (Figure 36.1). These studies show that increasing or decreasing the amount of fermentable carbohydrate in the diet has a profound effect on caries experience.
Other studies have shown that, in fact, it is not so much the amount of sugar that is eaten that is important but rather the frequency with which it is eaten and the length of time over which appreciable amounts of fermentable carbohydrate are present in the mouth. The Vipeholm experiment (page 133) clearly demonstrated that the consumption of sugar, especially in a sticky form between meals, promoted caries development.
Experiments in rodents, which do not normally develop caries, have shown that sucrose is the most cariogenic carbohydrate while other common mono- and di-saccharides and cooked starch are generally less cariogenic. Monkeys fed a typical child’s diet developed caries, and attempts are being made to assess the cariogenicity of foods so that snacks may be chosen for eating between meals which do not increase the risk of caries. Stephan curves prepared for each food show the ranking of a number of snacks according to their acidogenicity (Table 36.3). Sucrose-containing sweets, fruit drinks and sugared tea and coffee are among the most acidogenic snacks and a comparison of rat caries scores produced by different foods also showed that those containing sucrose were the most cariogenic. Perhaps surprisingly, many ‘natural’ foods were also highly cariogenic, particularly if they are acidic in nature. Honey, dates, raisins, grapes, apples and figs produced high caries scores; apples, grapes, iced lollies and cola drinks also produced acid erosion of the enamel surface. In general, starchy foods produced the least caries (bread alone) while a sugar supplement (bread and jam; sweet biscuits) increased the caries score in proportion to the sucrose content. Analyses have also shown that many unexpected foods contain sucrose, e.g. some tomato soups contain 10% sucrose.
Table 36.3
Ranking of different snack foods according to their minimum pH values achieved in the Stephan curve
| Snack | Minimum pH |
| Boiled sweet | 5·33 |
| Sugared coffee | 5·41 |
| Toffee | 5·43 |
| Orange drink | 5·51 |
| Plain biscuit | 5·56 |
| Sugared chewing gum | 5·59 |
| Chocolate-coated biscuit | 5·62 |
| Chocolate | 5·63 |
| Ice cream | 5·66 |
| Apple | 5·81 |
| Mars bar | 5·82 |
| Unsugared coffee | 6·10 |
| Ice-lolly (frozen) | 6·11 |
| Potato crisps | 619 |
| Bread and butter | 6·28 |
| Salted peanut | 6·50 |
| Strong cheese | 7·50 |
Adapted from Rugg-Gunn et al. (1978) British Dental Journal, 145, 95
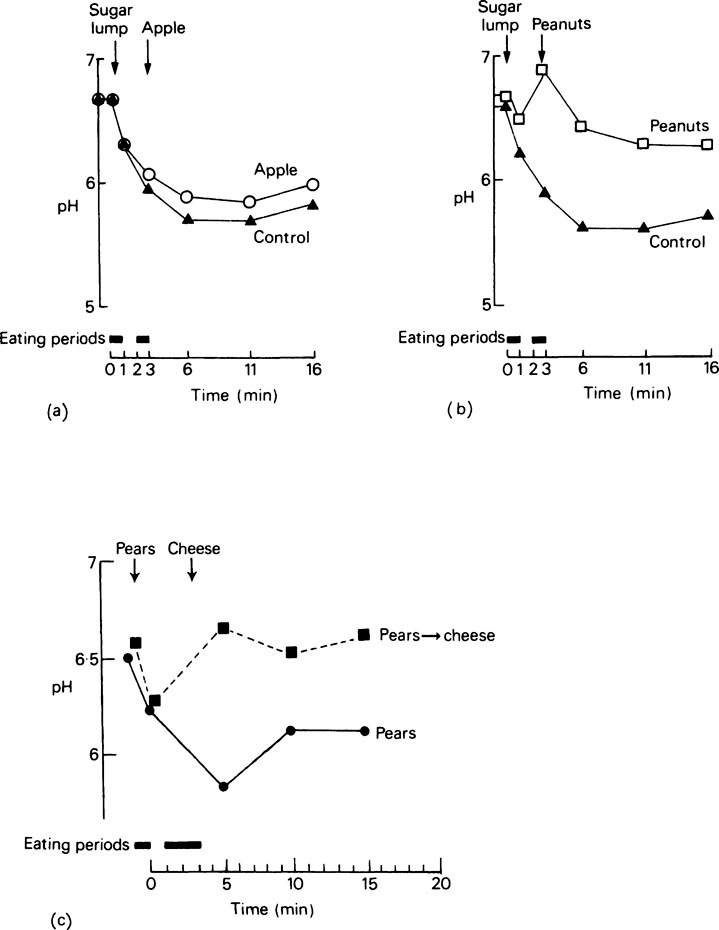
One of the main factors influencing the degree and duration of the fall in pH is the rate of salivary flow (page 481); if flow is stimulated during or immediately after sugar exposure the associated rise in salivary bicarbonate helps to buffer plaque acid and promotes a more rapid return of the pH to neutrality. Figure 36.2 shows the effects of saliva-stimulating foods such as an apple (a), and salted, roasted peanuts (b) on Stephan curves produced by a sugar lump and by strong cheese (c) given after tinned pears. Cheese eaten after sugar reduced caries in animals and it is possible that apart from reducing the acid the cheese also acts as a source of calcium and phosphate and other protective factors.
Sucrose is included in a wide variety of processed foods for reasons other than its sweet taste (page 134), and this often makes it difficult for the manufacturers to use an alternative sweetener. Sorbitol, mannitol and xylitol (page 136) have, however, been successfully incorporated into ‘sugar-free’ chewing gums and, since plaque bacteria metabolize them only very slowly, if at all, acid production is negligible. They have the additional advantage of stimulating salivary flow which causes a rise in pH and this may help in the remineralization of early lesions. Unfortunately, the consumption of large quantities of sugar alcohols leads to osmotic diarrhoea which has prevented their use in a wider range of confectionery. However, a whole range of alternative sweeteners is becoming available (page 135) and it is possible that some of them will be found to be suitable sucrose substitutes.
Maintenance of salivary flow and access
The importance of saliva in oral clearance, pH control, increased mineral ion availability and the provision of acid-neutralizing substrates such as urea and arginine peptides was considered in Chapter 35. In addition, saliva has specific microbial defence mechanisms which make the mouth a hostile place for bacteria. These, in the absence of fermentable carbohydrate, ensure that there is limited bacterial growth in the saliva.
(i) Saliva contains dissolved oxygen and this is the main factor limiting the growth of potentially pathogenic anaerobic organisms. These require a reduced oxygen content for growth and the redox potential has been shown to fall from +200 mV to −140 mV as plaque develops on a clean tooth surface. This is associated with a gradual increase in the plaque anaerobic community and is especially noticeable at the gingival margins and in periodontal pockets. Values which may be as low as −300 mV have been reported, and are to be expected, since spirochaetes which require a redox potential of −185 mV for growth can be isolated in this area.
Plaque possesses a range of oxygen tensions depending on the site and on salivary access. A good oxygen supply is important since hydrogen peroxide produced by bacterial oxidase reactions limits the growth of catalase-negative bacteria. These include many Gram-positive cocci and rods such as Actinomyces and lactobacilli. Hydrogen peroxide is also produced by neutrophils (derived mainly from the gingival crevice area) under aerobic conditions as a result of superoxide generation (page 159):
< ?xml:namespace prefix = "mml" />



This and other short-lived oxidation products also inhibit bacteria.
(ii) Saliva contains various proteins that inhibit bacterial growth; these include immunoglobulins synthesized locally and derived from the serum via the gingival fluid (page 477), the enzyme lysozyme (page 409) and transferrin, a Fe3+-binding protein which is capable of depriving organisms of this essential metal. The Gram-negative bacteria are particularly susceptible to iron deficiency but recent work has shown that the bactericidal effect is not a simple one since the inhibition of S. mutans is independent of iron deprivation. It has also been suggested that saliva contains specific agglutinins which cause clumping of bacteria, reducing their ability to colonize surfaces and favouring their removal by salivary wash-out. It also seems likely that all salivary organisms are coated with a variety of salivary glycoproteins in a non-specific manner.

The remaining two-thirds is mainly hydrophobic and it is this polar region, and particularly the two phosphoserine residues, which seem to provide a unique configuration for binding to nucleation and growth sites. Experiments have shown that a concentration of 1 μM, which is less than the concentration in saliva (2–6 μM), is sufficient to inhibit crystal growth completely. Salivary pyrophosphate has also been shown to be an effective inhibitor at low concentrations (7·5 μM) and it has been proposed that this and the peptide inhibitors act by binding to calcium phosphate nuclei and to growth sites on seed crystal surfaces thus preventing crystal growth (page 456). A number of other molecules also inhibit and it is not easy to define the characteristics which make an effective inhibitor; the minimum requirement seems to be a phosphate group and an adjacent acidic group which can either be another phosphate or a carboxylate group. An interesting example of a naturally produced inhibitor is phosphocitrate which is found in the urine and is synthesized within the mitochondrion:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


