The removal of impacted third molars teeth is one of the most common surgical procedures performed by oral and maxillofacial surgeons. In large part this is because of the high incidence of impacted teeth in modern societies that have effective public health measures and because contemporary science has identified the presence or likely development of pathology associated with a significant percentage of even asymptomatic third molars.
Eruption/impaction of third molars
- •
A tooth is impacted when it has failed to fully erupt into the oral cavity within its expected developmental time period and cannot reasonably be expected to do so.
- •
The most significant variable associated with third molar impaction is inadequate hard tissue space, with impacted third molars having space/crown width ratios of less than 1.
- •
The position and disposition of unerupted teeth is dynamic and unpredictable, with changes in position occurring well beyond the middle of the third decade.
- •
Proper periodontal support is not ensured even with eruption to the occlusal plane.
- •
Because there is no completely reliable way to predict pathologic changes associated with impacted teeth, they should be monitored periodically with clinical and radiographic examinations if a decision is made for retention.
A systematic preoperative clinical and imaging evaluation is critical in determining the need for and surgical approach to the removal of impacted third molars.
Classification of impacted teeth
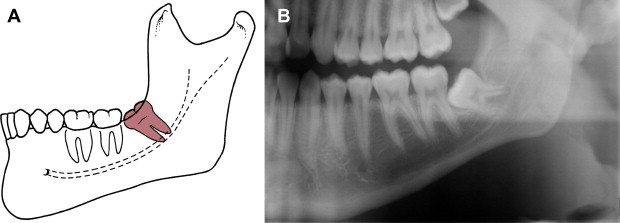
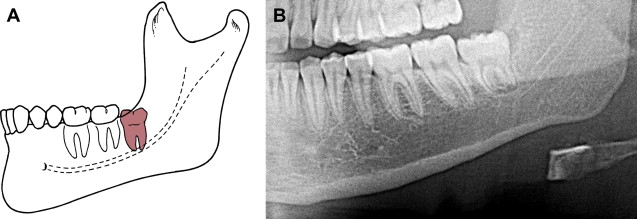
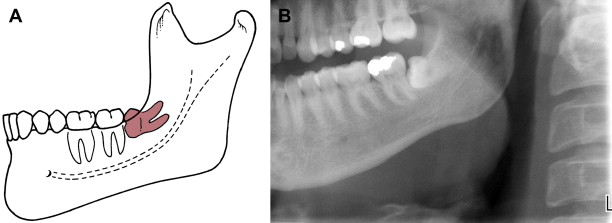
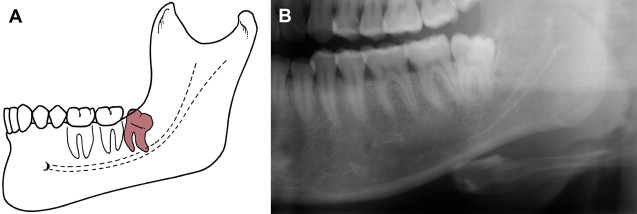
A variety of classification systems have been developed and assess the angulation of the impacted third molar, the relationship of the impacted tooth to the anterior border of the ramus and second molar, and the depth of the impaction. Examples of various impaction types are seen in Figs. 1–6 .
Several factors have been implicated in making the extraction process more complex are root morphology, the presence of a follicular sac (which provides more room for access to the tooth), and the position/condition of adjacent structures, such as the second molar.
Pell and Gregory Classification of Impacted Mandibular Third Molar Teeth
Based on relationship of anterior border of the ramus to teeth:
-
Class I: mandibular third molar has sufficient room anterior to anterior border of ramus to erupt
-
Class II: half of the impacted third molar is covered by the ramus
-
Class III: the impacted third molar is completely embedded in the ramus of the mandible
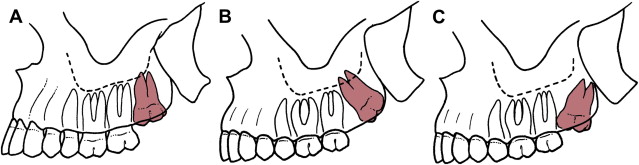
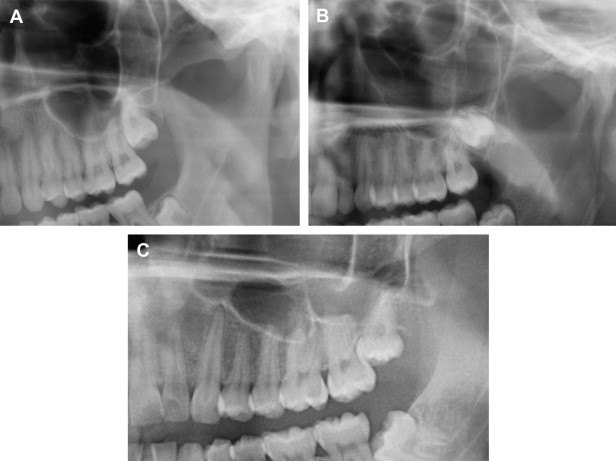
Pell and Gregory Classification of Impacted Maxillary Third Molar
Based on relationship of occlusal plane of second and third molars:
-
Class A: occlusal plane of third molar is the same as the second molar
-
Class B: occlusal plane of third molar is between the occlusal plane of the second molar and its cervical line
-
Class C: occlusal plane of the third molar is above the cervical line of the second molar
Winter Classification of Impacted Third Molars
Based on radiographic appearance of the third molar and its anatomic position in relation to the long axis of the adjacent second molar:
-
Mesioangular
-
Distoangular
-
Vertical
-
Horizontal
-
Buccoangular
-
Linguoanglar
-
Inverted
Other systems focus on the degree of impaction and the position of the tooth relative to the overlying tissues (soft and/or hard) ( Figs. 7–12 ).
American Dental Association Definitions
-
Removal impacted tooth–soft tissue: D7220
-
Occlusal surface of tooth covered by soft tissue: requires mucoperiosteal flap elevation
-
Removal impacted tooth–partially bony: D7230
-
Part of crown covered by bone; requires mucoperiosteal flap elevation and bone removal
-
Removal impacted tooth–completely bony: D7240
-
Most or all of crown covered by bone; requires flap elevation and bone removal
-
Removal of impacted tooth–completely bony with unusual surgical complications: D7241
-
Most or all of crown covered by bone; unusually difficult or complicated due to factors, such as nerve dissection required, separate closure of maxillary required, or aberrant tooth position
Classification of impacted teeth
A variety of classification systems have been developed and assess the angulation of the impacted third molar, the relationship of the impacted tooth to the anterior border of the ramus and second molar, and the depth of the impaction. Examples of various impaction types are seen in Figs. 1–6 .
Several factors have been implicated in making the extraction process more complex are root morphology, the presence of a follicular sac (which provides more room for access to the tooth), and the position/condition of adjacent structures, such as the second molar.
Pell and Gregory Classification of Impacted Mandibular Third Molar Teeth
Based on relationship of anterior border of the ramus to teeth:
-
Class I: mandibular third molar has sufficient room anterior to anterior border of ramus to erupt
-
Class II: half of the impacted third molar is covered by the ramus
-
Class III: the impacted third molar is completely embedded in the ramus of the mandible
Pell and Gregory Classification of Impacted Maxillary Third Molar
Based on relationship of occlusal plane of second and third molars:
-
Class A: occlusal plane of third molar is the same as the second molar
-
Class B: occlusal plane of third molar is between the occlusal plane of the second molar and its cervical line
-
Class C: occlusal plane of the third molar is above the cervical line of the second molar
Winter Classification of Impacted Third Molars
Based on radiographic appearance of the third molar and its anatomic position in relation to the long axis of the adjacent second molar:
-
Mesioangular
-
Distoangular
-
Vertical
-
Horizontal
-
Buccoangular
-
Linguoanglar
-
Inverted
Other systems focus on the degree of impaction and the position of the tooth relative to the overlying tissues (soft and/or hard) ( Figs. 7–12 ).
American Dental Association Definitions
-
Removal impacted tooth–soft tissue: D7220
-
Occlusal surface of tooth covered by soft tissue: requires mucoperiosteal flap elevation
-
Removal impacted tooth–partially bony: D7230
-
Part of crown covered by bone; requires mucoperiosteal flap elevation and bone removal
-
Removal impacted tooth–completely bony: D7240
-
Most or all of crown covered by bone; requires flap elevation and bone removal
-
Removal of impacted tooth–completely bony with unusual surgical complications: D7241
-
Most or all of crown covered by bone; unusually difficult or complicated due to factors, such as nerve dissection required, separate closure of maxillary required, or aberrant tooth position
Decision making for the removal of third molars
- •
The decision to remove an impacted tooth must be based on a careful evaluation of the potential benefits versus risks of treatment.
- •
In situations in which pathology is easy to identify, decision making is straightforward.
- •
It is often wise to remove third molars before the development of pathology and associated symptoms when the development of such is likely and at an age when surgery is straightforward.
- •
There are situations in which removal of impacted teeth is contraindicated, including advanced patient age, poor health, and potential for damage to adjacent structures.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


