History of the Procedure
Salivary gland surgery dates back to the sixteenth century. The anatomy of the parotid gland and the role of the main ducts were described in the midseventeenth century. The earliest references to “para-auricular swellings,” as the Greeks called them, described the findings associated with calculi and inflammation.
Between 1650 and 1750, salivary gland surgery was limited to the treatment of ranulas and oral calculi. The concept of surgical excision of a parotid tumor has been attributed to Bertrandi in 1802. The initial applications of this surgery included an extensive approach, which caused serious disfiguration and disability.
In about the 1850s, the focus shifted toward dissection and the intimate relationship between the facial nerve and the parotid gland. Attempts were made to perform the surgery with nerve preservation. John C. Warren, a physician, was the first to use ether inhalation anesthesia during resection of a parotid tumor in Boston in 1846. In 1892, Codreanu (a Romanian native) performed the first total parotidectomy with facial nerve preservation.
Before the 1950s, enucleation of benign neoplastic processes (e.g., pleomorphic adenoma) was the most common extirpative procedure; however, it was associated with elevated recurrence rates. The reason to perform enucleation rather than removal of the gland was concern regarding injury to the facial nerve.
In 1958, Beahrs and Adson eloquently described the relevant anatomy and surgical technique of current parotid gland surgery. They stressed the importance of surgical landmarks for avoiding injury to the facial nerve and advocated complete removal of the superficial portion of the parotid gland for noninvasive lesions confined to that location.
History of the Procedure
Salivary gland surgery dates back to the sixteenth century. The anatomy of the parotid gland and the role of the main ducts were described in the midseventeenth century. The earliest references to “para-auricular swellings,” as the Greeks called them, described the findings associated with calculi and inflammation.
Between 1650 and 1750, salivary gland surgery was limited to the treatment of ranulas and oral calculi. The concept of surgical excision of a parotid tumor has been attributed to Bertrandi in 1802. The initial applications of this surgery included an extensive approach, which caused serious disfiguration and disability.
In about the 1850s, the focus shifted toward dissection and the intimate relationship between the facial nerve and the parotid gland. Attempts were made to perform the surgery with nerve preservation. John C. Warren, a physician, was the first to use ether inhalation anesthesia during resection of a parotid tumor in Boston in 1846. In 1892, Codreanu (a Romanian native) performed the first total parotidectomy with facial nerve preservation.
Before the 1950s, enucleation of benign neoplastic processes (e.g., pleomorphic adenoma) was the most common extirpative procedure; however, it was associated with elevated recurrence rates. The reason to perform enucleation rather than removal of the gland was concern regarding injury to the facial nerve.
In 1958, Beahrs and Adson eloquently described the relevant anatomy and surgical technique of current parotid gland surgery. They stressed the importance of surgical landmarks for avoiding injury to the facial nerve and advocated complete removal of the superficial portion of the parotid gland for noninvasive lesions confined to that location.
Indications for the Use of the Procedure
An estimated 75% to 80% of parotid neoplasms are benign. Pleomorphic adenoma and Warthin’s tumor account for most of the neoplasms encountered. When malignancy is encountered, adenoid cystic carcinoma and mucoepidermoid carcinoma are approximately equally represented. Adenocarcinoma, acinic cell carcinoma, carcinoma ex-pleomorphic adenoma, squamous cell carcinoma, and malignant mixed tumor may occasionally be encountered. Lymphoma may arise in the intraparotid or paraparotid lymph nodes. The lymph nodes may also be sites of metastases from cutaneous squamous cell carcinoma and melanoma of the face and scalp. In rare cases, tumors may metastasize to parotid lymph nodes from distant sites.
Superficial parotidectomy is indicated for most benign and malignant tumors limited to the superficial lobe, for chronic sialadenitis, and as part of a lymphadenectomy for skin cancer of the scalp. Although some evidence suggests that certain lesions of the parotid gland can be treated or investigated with enucleation, it is the author’s opinion that this is an unsafe practice and should not be encouraged because of the risk of tumor spillage and recurrence, in addition to the increased risk of facial nerve injury during revision surgery. In certain situations, such as for the treatment of pleomorphic adenoma, the presence of a pseudocapsule allows the surgeon to remove less parotid parenchyma relative to tumor size, making partial superficial parotidectomy the procedure of choice. Tumors that extend into the deep lobe may require total parotidectomy.
Although the incisional parotid biopsy is the diagnostic procedure of choice for systemic disease involving the parotid, the superficial parotidectomy remains the minimal biopsy of choice for a mass suspected to be a neoplasm in the parotid.
Limitations and Contraindications
In about 20% of patients, the parotid gland is really one lobe with an accessory lobe along Stensen’s duct. The delineation of two lobes (the superficial lobe and the deep lobe), based on cranial nerve (CN) VII, is not so much anatomic as surgical.
The contents of the triangular space anterior and inferior to the auricle include, among others, numerous sensory and autonomic nerves, the external carotid artery and its branches, and the retromandibular vein.
The integrity of the facial nerve is among the most important considerations during treatment of parotid gland diseases ( Figure 88-1 ).
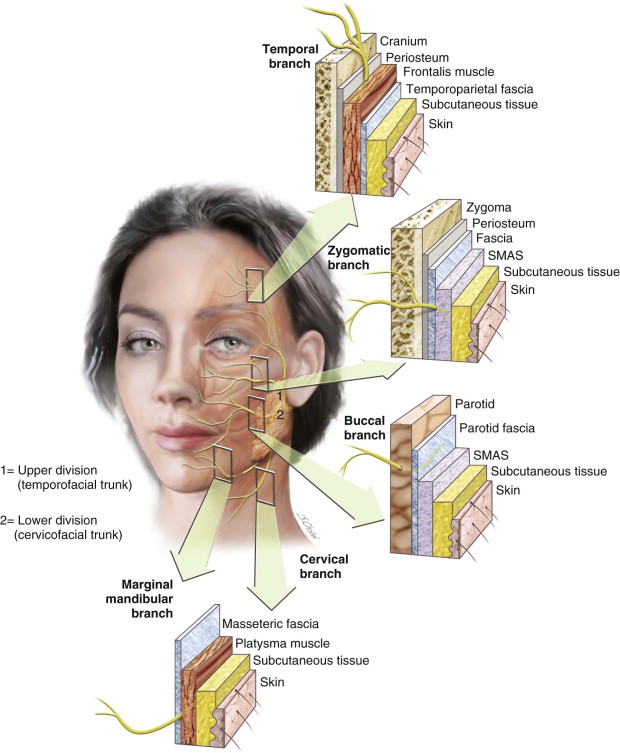
Davis et al. described six different facial nerve branching patterns, with no predominant pattern. In all types, the temporal and zygomatic branches arise from the upper division, and the cervical and marginal mandibular branches arise from the lower division. The major variations are in the origin of the buccal branch and the degree of cross-innervation between adjacent terminal branches. Such branching patterns have no particular significance during the surgical procedure, mainly because of the constancy of the main trunk as it enters the parotid gland.
Due to the benign nature of most parotid tumors, patients commonly expect intact motor function of the face after surgery. However, in addition to variations in nerve anatomy, the surgery may be further complicated by other factors, including previous surgery, infection, and a history of radiation therapy. The tumor’s size and type and its relation to the facial nerve may also increase the complexity of parotid surgery.
Poor general health is the only relative contraindication to parotid surgery. In general, the superficial parotidectomy procedure is well tolerated by patients, even those medically optimized to undergo general anesthesia.
Technique: Superficial Parotidectomy
Step 1:
Intubation
Oral endotracheal intubation with either a conventional tube or a right-angle endotracheal tube is preferred. The tube is secured with skin adhesive and tape. Wiring the tube to the existing dentition, if present, is another option. Avoidance of neuromuscular paralysis is important during the procedure to better identify the facial nerve.
Step 2:
Patient Positioning
Patient positioning is an important aspect of the surgical procedure. Proper positioning guarantees the surgeon’s comfort and helps avoid limitations in access. The patient is placed in the supine position on the operating room table; the head is extended and turned to the contralateral side. The table is then rotated 90 degrees, with the operative side of the patient away from the anesthesia machine.
Step 3:
Prepping and Draping
A sterile cotton ball is used to block the external auditory canal (EAC); this prevents tympanic membrane irritation in the event of Betadine accumulation after prepping. A corneal protector is then placed over the ipsilateral globe, and the face and neck are prepped with Betadine scrub. The entire operative field is then draped in a sterile fashion, exposing the patient’s ipsilateral eye, commissure, and chin to allow for visualization of facial movements during stimulation of the facial nerve ( Figure 88-2, A ).



Step 4:
Incision and Superficial Dissection
A marking pen is used to delineate a modified Blair incision, beginning in the preauricular region and extending into the upper aspect of the neck in a curvilinear fashion at the level of the hyoid bone, about 2 finger breadths below the angle of the mandible.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


