Introduction
The use of space maintainers after the premature loss of deciduous molars is routine in pediatric dentistry. However, there is a need for evidence offering a better scientific basis for prescribing these appliances. In this study, we aimed to assess dimensional changes in the dental arches after the premature loss of deciduous molars.
Methods
A sample of 55 children between 6 and 9 years of age with unilateral loss of either first or second molars was followed for 10 months by clinical examination, cast analysis, and radiographic analysis. The space in the extraction site, arch length, and hemi-perimeter of the extraction and control sides were measured. Intraexaminer agreement was high (0.990). The data were analyzed by using the F test (analysis of variance), Bonferroni test, least significant difference, and Student t test.
Results
Only the group of children with premature loss of the mandibular second deciduous molars exhibited significant dimensional alterations during the follow-up.
Conclusions
The findings emphasize a need for the judicious indication for space maintainers. The major effect on the dental arches occurred in the first 3 months after the extraction of the deciduous molars, indicating that these appliances should be fitted during this period.
Hutchinson and Davenport carried out the first investigations into the loss of space after the premature extraction of deciduous teeth. However, these studies had limitations, because of difficulties in the definition of the sample size and the methods of measurement of the dental arch and space related to the extraction. Liu carried out the first study to quantify the loss of space caused by the early extraction of deciduous molars. Comparing children with premature loss of deciduous molars with those without loss, the author found that the reduction in the arch space after the premature loss of the second deciduous molars in both the maxilla and the mandible had a greater negative effect on the occlusion than did the loss of the first deciduous molars.
These early studies relating to the association between the premature loss of deciduous molars and the loss of space in the extraction site attempted to explain this loss of space on the extraction side by the mesial movement of the first permanent molars, leading to crowding in the dental arch and impaction of the permanent successor. However, these studies also faced methodologic difficulties, such as the absence of a control group, data based on nonstandardized clinical charts, and inadequate criteria for selection of the sample. Most subsequent studies, including the most recent, have not associated the loss of space with the mesial movement of the permanent molar alone, but also to the distal movement of the deciduous canines. Table I summarizes these studies and their main results.
| Author/year | Country | n | Age (y) | Tooth | Data collection | Follow-up period | Main results |
|---|---|---|---|---|---|---|---|
| Northway et al, 1984 | Canada | 107 | 6 | First and second molars | Digitized plaster casts | 6 years | Greater reduction in cases of second molar extraction |
| Cuoghi et al, 1998 | Brazil | 31 | 6–10 | Mandibular first molar | Plaster casts | 6, 12, 18 months | Reduction in space from distal movement of deciduous canine |
| Lin and Chan, 1998 | China | 21 | 5–7 | Mandibular first molar | Plaster casts | 8 months | Reduction in space from distal movement of deciduous canine |
| Northway, 2000 | Canada | 13 | 6 | Maxillary first molar | Digitized plaster casts and panoramic x-rays | 6 years | Reduction in space from mesial movement of second deciduous molar |
| Padma Kumari and Retnakumari, 2006 | India | 30 | 6–9 | Maxillary first molar | Plaster casts | 2, 4, 6, 8 months | Reduction in space from distal movement of deciduous canine |
| Lin et al, 2007 | China | 19 | 4–7 | Maxillary first molar | Plaster casts | 6 months | Reduction in space from distal movement of deciduous canine and permanent incisors |
| Park et al, 2009 | Korea | 13 | 5–10 | Maxillary first molar | Digitized plaster casts | Mean of 12 months | No loss of space |
Although a number of authors have agreed that the premature loss of deciduous teeth has harmful consequences for the occlusion, some researchers have contested the indiscriminant use of space maintainers and suggested that tooth migration to the space left by the extraction depends on factors such as whether the tooth was lost or extracted, whether the extracted tooth was a first or second deciduous molar, the dental arch involved, the formation stage of the permanent successor, the occlusal relationship of the permanent molars, and the tooth eruption sequence in the patient.
Few studies have addressed the difference between the consequences of the early loss of the first and second deciduous molars in both dental arches. The literature offers little scientific evidence regarding the indications for space maintainers in the mixed dentition in the case of the premature loss of deciduous molars. Clinical studies have reported no statistically significant differences between the initial and final positions of the first permanent molar after the premature loss of the deciduous molars.
In this study, we aimed to assess space changes in the dental arches after premature loss of the first and second deciduous molars in Brazilian schoolchildren.
Material and methods
This study, carried out in Camaragibe, Pernambuco, Brazil, included boys and girls between 6 and 9 years of age enrolled in the municipal school system. The study received approval from the Ethics in Research Committee of the Pernambuco State University.
The inclusion criteria were unilateral extraction indicated for maxillary or mandibular first or second deciduous molars, all 4 incisors either erupted or in the process of eruption, first permanent molars erupted and in occlusion, premolars not erupted, deciduous canines in the arch of the extraction, and a deciduous canine adjoining the space left by the extraction throughout the entire follow-up period. The exclusion criteria were development syndromes or abnormalities, loss of other deciduous teeth in the arch to be studied, anodontia of the germ of the permanent successor, open bite, crossbite, and current or past orthodontic or orthopedic treatment.
For the determination of the sample size, a total of 1246 children were examined, of whom 87 fulfilled the inclusion criteria. However, after the radiographic examination, 24 children were excluded because of anodontia of the permanent teeth, ruling out extraction or the possibility of recovering teeth with caries through endodontics or restorative procedures. Thus, the study began with 63 children who fulfilled the eligibility criteria. At the end of the study, the sample was reduced to 55 children because of the loss of other dental elements or the child’s absence during the study period.
The study was carried out with a case group and a control group. The sampling unit was the dental hemi-arch, which was defined as one half of each arcade analyzed (left and right sides). The case group included hemi-arches with extraction of the first or second deciduous molar; the control group included contralateral hemi-arches with no extractions of the deciduous molars. The objective was to compare dimensional alterations over time in hemi-arches with and without the premature loss of deciduous molars under the same physiologic conditions in the same oral environment. Thus, the controls were identical to the cases in relation to confounding factors.
The following variables were analyzed.
- 1.
Dental space at the extraction site: for the cases of premature loss of the first deciduous molar, this space was measured in millimeters from the mesial surface of the second deciduous molar to the distal surface of the deciduous canine ( Fig , A ). For the cases of loss of the second molar, the space was measured from the mesial surface of the first permanent molar to the distal surface of the first deciduous molar ( Fig , B ).
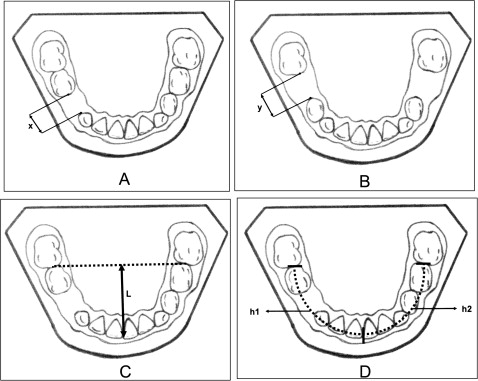
Fig Schematic drawings of measurements on the casts: A, dental space in the extraction site of the first deciduous molar ( x ); B, dental space in the extraction site of the second deciduous molar ( y ); C, length of the dental arch ( L ); D, hemi-perimeter of the dental arch of the extraction side ( h1 ) and the control side ( h2 ). - 2.
Length of the dental arch: this was determined from the orthogonal distance from the midpoint of the central incisors to a line tangential to the mesial surface of the first permanent molar ( Fig , C ).
- 3.
Hemi-perimeter of the dental arch: measured with a tin wire positioned from the midpoint of the mesial surface of the first permanent molar to the dental midline at the gingival margin, passing through the canine and the incisal edges of the canines and incisors, respectively. The measurement was determined for both sides (extraction and control) ( Fig , D ).
The data were collected through clinical examinations, radiographic analyses, and the analyses of the study casts. These methods were performed in sequence according to the work dynamic described below.
The aim of the clinical examination was to record data identifying the child, clinically verify the indication for extraction with a dental headlamp and wooden tongue depressors, and assess the molar relationship.
After the clinical examination, periapical x-rays were taken of the teeth indicated for extraction. After analysis of the x-rays and confirmation of the diagnosis, the extractions were scheduled. The diagnostic criterion for extraction was a high degree of decay of the tooth crown by caries, with the impossibility of direct or indirect reconstruction or restoration.
All patients had molding of the dental arches before extraction and at 3, 6, and 10 months after the extractions. The measurements on the casts were made by 1 examiner (M.C.B.M.) using a digital caliper accurate to 0.02 mm (Mitutoyo Sul Americana, São Paulo, Brazil). To minimize the possibility of measurement errors, all measurements were made twice by the same examiner on separate occasions. In the determination of intraexaminer agreement, the concordance correlation coefficients were high for all measurements and all evaluation times (above 0.990).
To minimize the risk of complications or any other harm to the patients, the extractions were carefully planned and executed. Children with other dental needs were treated.
Statistical analysis
The data were analyzed by using the Statistical Package for the Social Sciences (version 15; SPSS, Chicago, Ill). The margin of error used in the interpretation of the statistical tests was 5.0%, and 95% CI values were obtained. The following statistical tests were used: F test (analysis of variance [ANOVA]) for repeated measurements, Bonferroni comparisons for significant differences, least significant difference for cases of incoherence between the results of the paired comparisons, and Student t tests with equal and unequal variances.
Results
Most of the children were girls (69.1%) between 8 and 9 years of age (63.6%). There was a greater frequency of extraction of the mandibular second molar (40.0%; 22 subjects), followed by the maxillary second molar (23.6%; 13 subjects), the mandibular first molar (21.8%; 12 subjects), and the maxillary first molar (14.6%; 8 subjects). Thus, the stratification of the sample resulted in insufficient power of analysis for the maxillary first molar group.
The sample was also assessed in relation to crowding. Only 3 children exhibited maxillary crowding greater than 4 mm in the arch with loss of the deciduous tooth. As a result, this variable was not considered in the analysis, because crowding of less than 4 mm in this age group (transitional period of the mixed dentition) can be considered physiologic.
The Tables display the measurements of the space left by the extraction and arch length in the initial evaluation as well as at 3, 6, and 10 months after the extractions. The differences in the pattern of changes in the dental arches are also shown for each group of teeth extracted between successive evaluations: D1 (initial-3 months), D2 (3-6 months), and D3 (6-10 months). In all Tables, a positive value denotes a decrease in the measurement, and a negative value denotes an increase in the measurement. For Bonferroni paired comparisons, the different letters in parentheses denote a significant difference between the corresponding evaluations.
Table II displays the results of the analysis of the space left by the extraction and the arch length at the 4 evaluation times for each group of teeth extracted, and Table III gives the differences in the pattern of changes between successive evaluations of the measurement of the extraction spaces and arch lengths per tooth group.
| Measurement | Tooth group | Evaluation (mm) | P value | |||
|---|---|---|---|---|---|---|
| Initial | 3 months | 6 months | 10 months | |||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Extraction space | Maxillary first molar | 7.3 ± 0.8 | 7.0 ± 0.6 | 7.0 ± 0.5 | 7.1 ± 0.5 | P ∗ = 0.284 |
| Mandibular first molar | 8.0 ± 0.7 | 7.8 ± 0.8 | 7.9 ± 0.9 | 7.9 ± 0.9 | P ∗ = 0.496 | |
| Maxillary second molar | 8.5 ± 1.2 (A) | 7.3 ± 1.1 (BC) | 7.4 ± 0.8 (C) | 7.8 ± 0.5 (AB) | P ∗ <0.001 † | |
| Mandibular second molar | 9.6 ± 0.7 (A) | 8.8 ± 0.7 (B) | 8.5 ± 0.7 (C) | 8.4 ± 0.8 (C) | P ∗ <0.001 † | |
| Arch length | Maxillary first molar | 28.3 ± 1.2 | 28.3 ± 1.3 | 28.5 ± 1.7 | 30.0 ± 4.0 | P ∗ = 0.211 |
| Mandibular first molar | 24.8 ± 2.1 | 24.9 ± 1.8 | 24.9 ± 1.9 | 24.9 ± 1.8 | P ∗ = 0.864 | |
| Maxillary second molar | 30.1 ± 2.1 | 29.7 ± 2.2 | 29.7 ± 2.2 | 29.9 ± 2.1 | P ∗ = 0.095 | |
| Mandibular second molar | 25.8 ± 1.5 (A) | 25.6 ± 1.4 (AB) | 25.5 ± 1.5 (B) | 25.5 ± 1.4 (B) | P ∗ = 0.032 † | |
| Measurement | Tooth group | Differences (mm) | P value | ||
|---|---|---|---|---|---|
| D1: initial-3 months | D2: 3-6 months | D3: 6-10 months | |||
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| Extraction space | Maxillary first molar | 0.3 ± 0.5 | 0.0 ± 0.4 | −0.1 ± 0.3 | P ∗ = 0.193 |
| Mandibular first molar | 0.2 ± 0.4 | −0.1 ± 0.4 | 0.0 ± 0.5 | P ∗ = 0.294 | |
| Maxillary second molar | 1.2 ± 0.8 (A) | −0.1 ± 0.5 (B) | −0.4 ± 0.5 (B) | P I ∗ <0.001 † | |
| Mandibular second molar | 0.8 ± 0.7 (A) | 0.3 ± 0.4 (B) | 0.1 ± 0.3 (B) | P I ∗ <0.001 † | |
| Arch length | Maxillary first molar | 0.0 ± 0.4 | −0.2 ± 0.8 | −1.5 ± 3.1 | P ∗ = 0.268 |
| Mandibular first molar | −0.1 ± 0.7 | 0.0 ± 0.5 | 0.0 ± 0.6 | P ∗ = 0.954 | |
| Maxillary second molar | 0.4 ± 0.5 (A) | 0.0 ± 0.3 (B) | −0.2 ± 0.4 (B) | P II ∗ = 0.016 † | |
| Mandibular second molar | 0.2 ± 0.5 | 0.1 ± 0.4 | −0.0 ± 0.4 | P ∗ = 0.087 | |
It was observed that the mean measurements of the extraction space varied, but there was a significant space reduction only in the group of second deciduous molars ( Table II ). With regard to the extraction space, the only teeth with statistically significant differences between evaluations were the maxillary and mandibular second molars ( P <0.001).
Regarding the maxillary second deciduous molars, there was a reduction and a subsequent increase in the mean extraction space, with a significant difference between the initial evaluation and both the 3-month and 6-month evaluations ( P <0.001). Between 6 and 10 months, there was an increase in the mean measurement of this space, with a statistically significant difference between the 2 evaluation times ( Table II ). These results were confirmed in Table III , which shows a statistically significant difference in mean extraction space in the D1 ( A ) successive evaluations compared with the mean D2 ( B ) and D3 ( B ) values. This demonstrates that this group of teeth underwent the greatest loss of space in the first 3 months after extraction, with an increase in this space in the subsequent months.
For the mandibular second deciduous molars, the mean measurement of the extraction space underwent a significant reduction between the initial evaluation and the 3 subsequent evaluations ( P <0.001). This reduction was greatest at 3 months and continued to the tenth month (albeit to a lesser degree), with no recovery of the original space ( Table II ). Table III confirmed this result, demonstrating that this group of teeth also underwent the greatest loss of space in the first 3 months after the extractions, with continued loss (albeit to a lesser degree) in the subsequent months.
With regard to arch length, only children with premature loss of the mandibular second deciduous molars exhibited a statistically significant difference throughout the study ( P = 0.032). In this group, mean arch length was greatest at the initial evaluation, with significant differences between the initial evaluation ( A ) and both the 6-month ( B ) and 10-month ( B ) evaluations, as determined by the Bonferroni paired comparison analysis ( Table II ).
The group with loss of the maxillary second deciduous molars showed a statistically different pattern of change of arch length throughout the study ( P = 0.016). In this group, there was a statistically significant difference in mean arch length in the D1 ( A ) evaluations compared with the mean D2 ( B ) and D3 ( B ) values. This demonstrated that this group of teeth experienced the most significant changes in this measurement in the first 3 months after the extractions ( Table III ).
Table IV displays the differences in the relative changes in extraction space and arch length between the 2 arches after the extraction of the second molars. There was a significant difference in the pattern of change between the arches only after the third month of follow-up. Between the 3-month and 6-month evaluations ( P = 0.023) and between the 6-month and 10-month evaluations ( P <0.001), the maxillary second deciduous molar tended to recover the space lost at the extraction site, whereas the mandibular second deciduous molar continued the pattern of loss.
| Measurement | Tooth group | Differences (mm) | ||
|---|---|---|---|---|
| D1: initial-3 months | D2: 3-6 months | D3: 6-10 months | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Extraction space | Maxillary second molar | 1.2 ± 0.8 | −0.1 ± 0.5 | −0.4 ± 0.5 |
| Mandibular second molar | 0.8 ± 0.7 | 0.3 ± 0.4 | 0.1 ± 0.3 | |
| P value | P ∗ = 0.152 | P ∗ = 0.023 † | P ∗ <0.001 † | |
| Arch length | Maxillary second molar | 0.4 ± 0.5 | 0.0 ± 0.3 | −0.2 ± 0.4 |
| Mandibular second molar | 0.2 ± 0.5 | 0.1 ± 0.4 | 0.0 ± 0.4 | |
| P value | P ∗ = 0.421 | P ∗ = 0.321 | P ∗ = 0.455 | |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


