This case report illustrates the use of miniscrews to treat a patient with an open bite caused by mandibular condylar fractures. The patient was 36 years old when she visited our hospital with a chief complaint of difficulty with chewing. She had suffered condylar and maxillary bone fractures in a traffic accident 6 months before her visit. She had an anterior open bite and Angle Class II molar relationships. Her mandibular midline was deviated to the right relative to the maxilla. The cephalometric analysis showed a skeletal Class II relationship. Titanium miniscrews were implanted in the bilateral maxillary buccal areas. The maxillary dentition was retracted and intruded by using elastomeric chains and miniscrews. After this treatment, an Angle Class I molar relationship was achieved, her overjet and overbite became ideal, and a good facial appearance was obtained. The total active orthodontic treatment period was 33 months. Treating an open bite with molar intrusion often leads to counterclockwise rotation of the mandible; however, in this patient, the mandible was moved anteriorly and upward. We believe that this movement was caused by the patient’s condylar fractures and the subsequent remodeling. Although there was some relapse, our results suggest that implant anchorage is useful for correcting anterior open bites originating from condylar fractures.
Fractures of the mandibular condylar and articular joints represent 20% to 52% of all mandibular fractures and thus are among the most common facial fractures. Nondislocated mandibular condylar fractures and condylar fractures in children can be successfully treated with conservative treatment. However, in adults, mandibular displacement caused by a condylar fracture can cause complications such as anterior open bite, discrepancies in centric relationship and maximal intercuspation, mandibular posterior displacement, decreased posterior facial height, and increased anterior facial height. To treat mandibular displacement immediately after an injury, intermaxillary fixation and prosthetic or surgical methods, such as condylectomy and mandibular osteotomy, have been developed. However, if a malocclusion remains after healing of the condylar fracture, routine open reduction and fixation of the condylar fracture is not indicated. Rather, the residual malocclusion can be corrected with orthognathic surgery.
Recently, molar control with implant anchorage has been established as a new treatment method for anterior open bite. However, there are no reports about the treatment of open bite from a condylar fracture.
In this report, we describe a patient with an open bite involving an Angle Class II and skeletal Class II malocclusion caused by bilateral condylar fractures; it was treated by using orthodontic miniscrews as anchorage, without premolar extractions or surgical orthodontics, and the result was a good facial profile and occlusal relationship. Although improvement in the facial profile was retained, we found a slight decrease of her overbite at 18 months after treatment.
Diagnosis and etiology
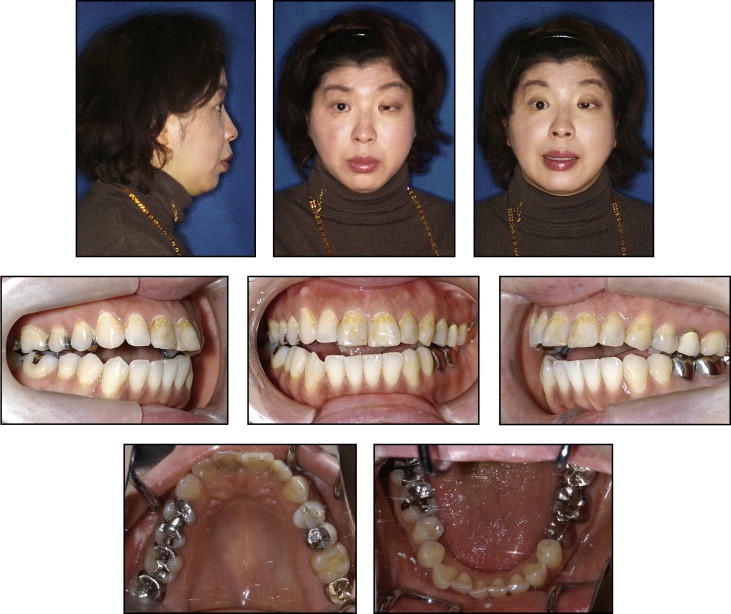
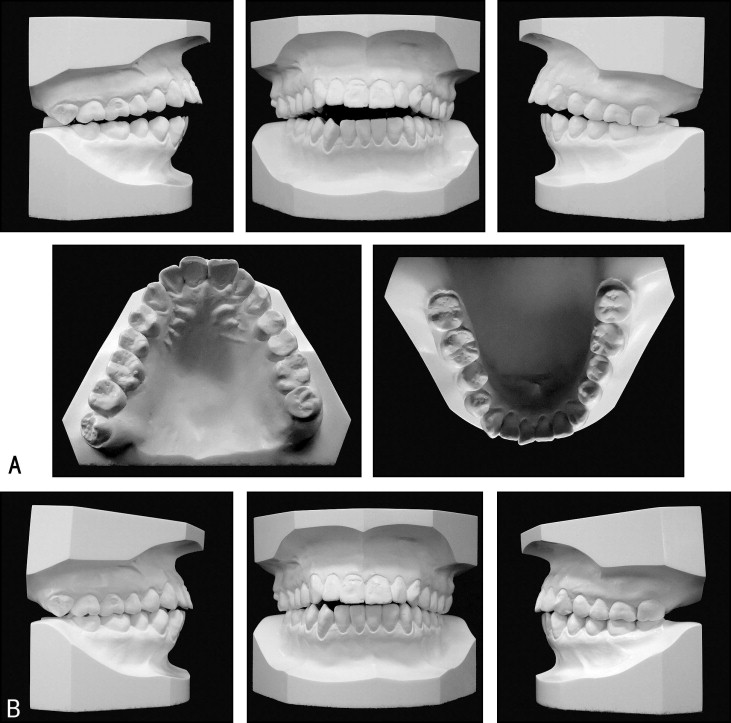
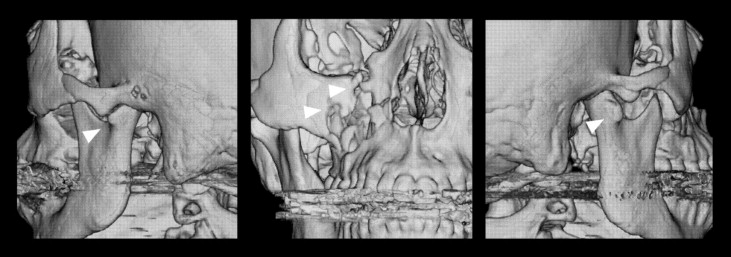
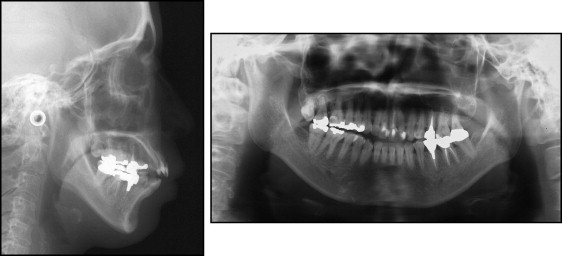
Our female patient was 36 years 0 months of age at the first examination. She visited our university dental hospital with a chief complaint of chewing difficulties associated with the anterior teeth. She had injured her head and face in a traffic accident 6 months before her visit. Initially, her frontal facial appearance showed left deviation of the mandible, and her lateral profile exhibited posterior mandibular positioning. Tongue thrusting was observed during conversation. The dental midline of her mandible was deviated 2 mm to the left relative to the facial midline. Her molars showed occlusal interferences, and her anteroposterior relationship was Angle Class II, with an overjet of 5.2 mm and an overbite of −4.0 mm ( Figs 1 and 2 , A ). Both dental arches were symmetric, with U-shaped arches. The dental casts showed arch length discrepancies of −1.0 and −1.5 mm in the maxilla and the mandible, respectively. Assuming that the initial dental cast before the trauma had an Angle Class I relationship, the occlusal appearance of the maxilla and the mandible was good except for the shallow overjet of the incisors ( Fig 2 , B ). On the pretreatment 3-dimensional computed tomography images, we found that both condyles were deformed; however, the fracture lines were not clear ( Fig 3 ). The results of an examination with a 3-dimensional, 6 degree of freedom jaw movement measurement apparatus (Gnathohexagraph system, version 1.31; Ono Sokki, Kanagawa, Japan) showed that the movements of the bilateral condyles during lateral sliding movements and anterior movements were irregular, with the incisal path unstable. With an occlusal force recording system (Dental Prescale and Occluzer; Fuji Film, Tokyo, Japan), her maximum occlusal force was found to be relatively weak (201 N). No impacted teeth were seen on the panoramic radiograph ( Fig 4 ). The cephalometric analysis showed that she had a skeletal Class II anteroposterior jaw relationship with an ANB angle of 8.3°. Vertically, the mandibular plane angle was 46.9°, which differed from the mean value for Japanese women by more than 1 SD. Her gonial angle was within the standard range. The axial inclination of her maxillary and mandibular incisors was less than –1 SD from the mean value for Japanese women, her L1-Mp angle was more than 1 SD from the mean value for Japanese women, and the distance between the palatal plane and the maxillary first molars was 27.2 mm, which was 3.4 mm larger than the mean value for Japanese women ( Table ).
| Mean | SD | Pretreatment | Posttreatment | 18 months posttreatment | |
|---|---|---|---|---|---|
| Angular analysis (°) | |||||
| SNA | 80.8 | 3.61 | 82.4 | 82.5 | 82.5 |
| SNB | 77.9 | 4.54 | 74.2 | 74.6 | 75.4 |
| ANB | 2.8 | 2.44 | 8.3 | 7.9 | 7.1 |
| Mp-SN | 37.1 | 4.64 | 46.9 | 46.8 | 45.6 |
| Gonial angle | 122.1 | 5.29 | 127.4 | 128.5 | 126.5 |
| U1-SN | 105.9 | 8.79 | 101.5 | 97.0 | 97.6 |
| L1-Mp | 93.4 | 6.77 | 100.4 | 100.0 | 99.7 |
| IIA | 123.6 | 10.64 | 111.2 | 116.2 | 117.1 |
| Occlusal plane | 16.9 | 4.4 | 20.2 | 24.3 | 23.9 |
| Linear analysis (mm) | |||||
| PTM-A/PP | 47.9 | 2.8 | 49.7 | 48.2 | 47.8 |
| PTM-ANS/PP | 52.1 | 3.04 | 53.4 | 51.8 | 50.1 |
| Go-Me | 71.4 | 4.14 | 69.3 | 69.5 | 69.6 |
| Ar-Go | 47.3 | 3.33 | 46.7 | 44.4 | 45.3 |
| Ar-Me | 106.6 | 5.74 | 106.5 | 104.6 | 105.1 |
| U6/PP | 24.6 | 2.0 | 27.2 | 23.7 | 24.6 |
| U1/PP | 31 | 2.34 | 33.0 | 30.5 | 31.8 |
| L6/Mp | 32.9 | 2.5 | 33.4 | 34.0 | 34.0 |
| L1/Mp | 44.2 | 2.68 | 45.6 | 45.3 | 44.9 |
| Overjet | 3.1 | 1.07 | 5.2 | 1.3 | 3.5 |
| Overbite | 3.3 | 1.89 | −4.0 | 1.0 | −0.5 |
Treatment objectives
We diagnosed the patient with an Angle Class II malocclusion, a skeletal open bite, and a skeletal Class II relationship. The treatment objectives were to correct her open bite and midline deviation, establish an ideal incisor relationship, achieve acceptable occlusion with a favorable functional Class I occlusion, and correct her convex facial profile. As her maxillary molars were extruded, we planned to implant miniscrews in the buccal area of the maxillary molars to provide skeletal anchorage for their intrusion and distal movement.
Treatment objectives
We diagnosed the patient with an Angle Class II malocclusion, a skeletal open bite, and a skeletal Class II relationship. The treatment objectives were to correct her open bite and midline deviation, establish an ideal incisor relationship, achieve acceptable occlusion with a favorable functional Class I occlusion, and correct her convex facial profile. As her maxillary molars were extruded, we planned to implant miniscrews in the buccal area of the maxillary molars to provide skeletal anchorage for their intrusion and distal movement.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


