Class II malocclusion is a challenging anomaly in orthodontic practice. Various types of functional appliances are used to correct Class II skeletal and occlusal disharmonies in growing patients, including the Twin-block. We used a modified sagittal-guidance Twin-block appliance combined with a fixed appliance and microimplant anchorage to treat a 13-year-old Chinese boy with a severe skeletal Class II malocclusion and mandibular retrognathia. Normal overjet and a Class I molar relationship were achieved because of the advancement of mandibular development, the restriction of maxillary growth, and dentoalveolar modifications in both the maxilla and the mandible. Favorable skeletal, dental, and soft tissue relationships were accomplished after 24 months of treatment. After 2 years of retention, the results remained stable.
Highlights
- •
A 13-year-old boy had severe skeletal Class II malocclusion and mandibular retrognathia.
- •
He was treated with sagittal-guidance Twin-block, fixed appliances, microimplant anchorage.
- •
Normal overjet and a Class I molar relationship were achieved.
- •
Favorable skeletal, dental, and soft tissue relationships were accomplished in 24 months.
- •
After 2 years of retention, the results remained stable.
Class II malocclusion is a challenging anomaly in orthodontic practice. The development of this malocclusion is due to mandibular retrognathia, maxillary protrusion, or both. It has been reported that retrusion of the mandible is the factor that most commonly contributes to a Class II malocclusion.
Various types of functional appliances (eg, activator, bionator, Fränkel, and Herbst) are used for the correction of Class II skeletal and occlusal disharmonies in growing patients. Over recent decades, Twin-block appliances, which were originally developed by Clark in the late 1970s, have increased in popularity.
In this case report, we used a renovated sagittal-guidance Twin-block appliance (SGTB) combined with a fixed appliance and microimplant anchorage for the treatment of a 13-year-old Chinese boy with a severe skeletal Class II malocclusion and mandibular retrognathia.
The SGTB consists of a bonded maxillary component and a mandibular removable counterpart. The maxillary component, which was bonded to the maxilla, has occlusal planes that cover the bilateral buccal dentition and often has a screw expansioner incorporated palatally. The mandibular piece, which is removable via Adams clasps on the first premolars and the first molars and ball clasps between the mandibular incisors for retention, has occlusal planes that bilaterally cover only the area of the premolars combined with a lingual acrylic pad that extends posteriorly. The angulation of the interface between the upper and lower occlusal planes is 70°. Two brackets are embedded into the buccal facade of the upper occlusal planes and serve as anchorage for the further placement of a maxillary partial fixed appliance.
The cephalometric analysis of Pancherz showed that the normal overjet and a Class I molar relationship were achieved because of the advancement of mandibular development, the restriction of maxillary growth, and dentoalveolar modifications in both the maxilla and the mandible. Favorable skeletal, dental, and soft tissue relationships were accomplished after 24 months treatment. After 2 years of retention, the stability of the treatment was pronounced.
Diagnosis and etiology
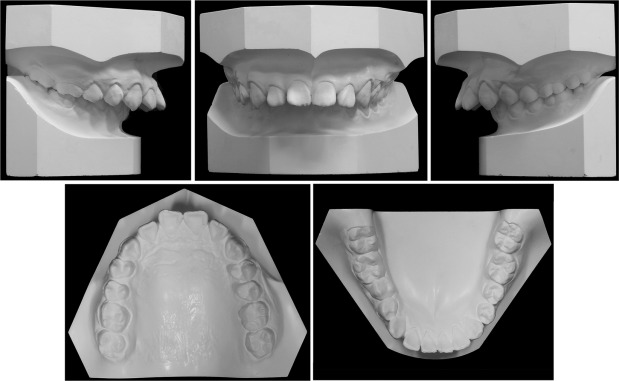
The patient was a 13-year-old Chinese boy with a convex facial profile, protrusive and everted lips, and a deep mentolabial fold. The frontal view did not show any facial asymmetry or deviation between the dental and facial midlines ( Fig 1 ).

Intraoral, dental cast, and 3-dimensional (3D) model examinations showed full-unit Class II molar relationships on both sides. A deep overjet of 12.7 mm, a complete deep overbite, and a resultant deep curve of Spee were also found. Furthermore, there was a scissors-bite of the premolars on the right side. The maxillary arch had spread spacings of 4.5 mm ( Figs 1 and 2 ).
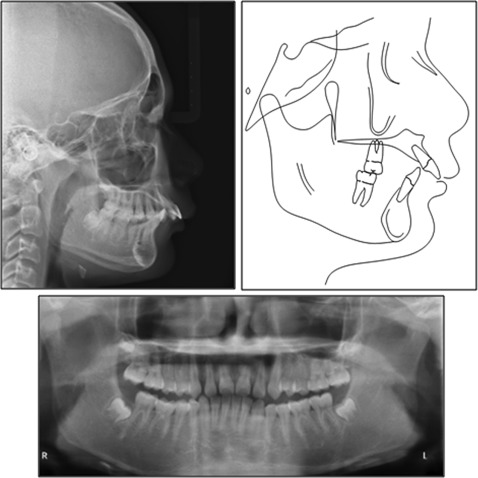
The lateral cephalometric analysis showed a Class II skeletal pattern that resulted from maxillary protrusion and mandibular retrusion (ANB, 7.6°; Wits appraisal, 8.8 mm) and a decreased mandibular plane angle (MP-FH, 18.3°). Both the maxillary and mandibular incisors were labially proclined (U1-SN, 122.2°; L1-MP, 109.9°). A panoramic radiograph showed root morphology that appeared normal, and 4 third molars were developing. Examinations of the cephalometric and cervical vertebrae suggested that the patient was in a pubertal growth spurt ( Fig 3 ; Table I ), which indicated optimal timing for orthopedic therapy for a Class II disharmony.
| Variable | Pretreatment | After Twin-block appliance | Posttreatment | Δ |
|---|---|---|---|---|
| SNA (°) | 85.3 | 85.2 | 85.3 | 0 |
| SNB (°) | 77.8 | 79.5 | 80.9 | 3.1 |
| ANB (°) | 7.5 | 5.7 | 4.4 | −3.1 |
| Wits (mm) | 8.8 | 5.4 | 4.0 | −4.8 |
| ANS-PNS (mm) | 52.6 | 51.8 | 51.7 | −0.9 |
| Go-Me (mm) | 74.6 | 75.9 | 77.4 | 2.8 |
| Ar-Go (mm) | 51.4 | 53.8 | 55.1 | 3.7 |
| ANS-Me (mm) | 64.1 | 66.6 | 66.0 | 1.9 |
| MP-FH (°) | 18.3 | 19.2 | 18.5 | 0.2 |
| U1-L1 (°) | 104.3 | 116.6 | 122.6 | 18.3 |
| U1-SN (°) | 122.2 | 108.4 | 104.6 | −17.6 |
| L1-MP (°) | 109.9 | 112.2 | 112.1 | 2.2 |
| Overjet (mm) | 12.7 | 4.8 | 2.8 | −9.9 |
| Overbite (mm) | 6.1 | 3.7 | 2.8 | −3.3 |
No symptoms of temporomandibular disorder were detected.
Based on these findings, the patient was diagnosed with a Class II Division 1 malocclusion, a low mandibular plane angle, a deep overbite, a deep overjet, and a localized scissors-bite.
Treatment objectives
The treatment objectives for this patient were the following: (1) amend the skeletal discrepancy with a SGTB, (2) retract the maxillary front teeth, (3) create ideal overjet and overbite, (4) correct the scissors-bite of the premolars on the right side, (5) improve the facial profile, and (6) ultimately achieve long-term stability.
Treatment objectives
The treatment objectives for this patient were the following: (1) amend the skeletal discrepancy with a SGTB, (2) retract the maxillary front teeth, (3) create ideal overjet and overbite, (4) correct the scissors-bite of the premolars on the right side, (5) improve the facial profile, and (6) ultimately achieve long-term stability.
Treatment alternatives
Orthopedic treatment with headgear alone to distalize the maxillary buccal segment could have corrected the molar relationship and reduced the overjet and may also have restrained the maxilla, but the efficacies of these removable appliances and headgear depend on patient compliance. Moreover, the unesthetic appearance can embarrass the patient and result in poor cooperation.
Camouflage therapy by removing the maxillary premolars in patients with mandibular retrognathia requires a more thorough assessment ; otherwise, it can lead to detrimental changes in the soft tissue profile.
The treatment of Class II adolescent patients requires careful diagnosis and treatment planning. The family was shown a simulation of the results of protruding the mandible forward, and they preferred this profile.
Treatment progress
The patient and his parents agreed with the treatment plan after receiving detailed explanations about the SGTB, microimplant anchorage, and related clinical procedures. This protocol was accepted by the patient’s family and approved by the ethics committee of Shanghai Ninth People’s Hospital.
The SGTB appliance was issued after oral hygiene instructions and scaling ( Fig 4 ). For the spaced and proclined maxillary incisors, early retraction of the anterior teeth was selected. Therefore, 2 embedded preadjusted straight-wire brackets for the buccal surfaces of the maxillary first premolars were designed, and the maxillary component was fixed to the arch to serve as a strong anchorage for anterior teeth alignment. The patient was instructed to wear the SGTB 24 hours per day and perform musculature exercises by pressing his lips together as much as possible.

The brackets were bonded on the maxillary front teeth in the fourth month, and a 0.012-in nickel-titanium wire was engaged for the initial alignment ( Fig 5 ). After 8 months of treatment, the maxillary frontal segment was retracted backward with an 0.018-in stainless steel archwire. The bonded maxillary device served as solid anchorage for the retraction of the anterior teeth ( Fig 6 ). At this time, the spaces between the maxillary canines and the acrylic blocks were approximately 2 mm, which indicated that the SGTB appliance produced favorable molar distalization in the maxillary buccal segment.


