Introduction
The purpose of this study was to determine the relationship between the length of the lingual frenulum and craniofacial morphology and test the hypothesis that skeletal Class III malocclusion is related to tongue-tie, in which the lingual frenulum is short and restricts the mobility of the tongue.
Methods
The sample consisted of 50 skeletal Class I patients (0° < ANB angle < 4°), 50 skeletal Class II patients (ANB angle > 4°), and 50 skeletal Class III patients (ANB angle <0°). Direct and indirect measuring methods were used to quantify the length of the lingual frenulum. The median lingual frenulum length was measured directly with a lingual frenulum ruler. It was evaluated indirectly by measuring the differences between the maximum mouth opening with and without the tip of the tongue touching the incisive papilla. A lateral cephalogram was taken for each subject and a computerized cephalometric analysis was used to assess the cranial morphology. Analysis of variance (ANOVA) was used to compare the differences among the 3 groups. The Pearson correlation analysis was used to detect any relationship between the lingual frenulum length and cephalometric variables.
Results
The median lingual frenulum length was significantly longer in the skeletal Class III subjects compared with the skeletal Class I and Class II subjects. The maximum opening of the mouth was significantly reduced in the skeletal Class III subjects compared with Class I and Class II subjects. Significant correlations were also found among the median lingual frenulum length, maximum mouth opening reduction, and the cephalometric variables such as the SNB and ANB angles, Wits appraisal, mandibular length, and the interincisal angle.
Conclusions
The present study supports the hypothesis that skeletal Class III malocclusion is related to long median lingual frenulum or a tongue-tie tendency. Patients diagnosed with tongue-tie might have a tendency toward skeletal Class III malocclusion.
The relationship between tongue posture and skeletal structures of the face is an essential element in understanding the growth and development of craniofacial structures, the etiology of malocclusions, and the prediction of stability after orthodontic treatment.
While it has been suggested that the mandible grows to a genetically predetermined size and shape, it also appears that a range of physiologic, pathologic, and mechanical factors can influence this growth. Proffit suggested that the teeth and alveolus lie in a balanced position between the cheeks, lips, and tongue; however, research has shown that the tongue is more powerful. Proffit and Mason have suggested that the tongue posture could be more influential than its action.
Many studies have evaluated the interaction between the position of the tongue and malocclusion. Tuerk and Lubit suggested that restriction of the free upward and backward movement of the tongue may result in an exaggerated tongue thrusting against the anterior body of the mandible, producing malocclusions such as anterior open bite and mandibular prognathism. Whitman and Rankow suggested that nearly all Class III patients have genioglossus muscle fibers that are too short or are positioned abnormally low. Hopkin studied the tongue posture and found that the tongue position is highest in Class II, lowest in Class III, and intermediate in Class I malocclusions.
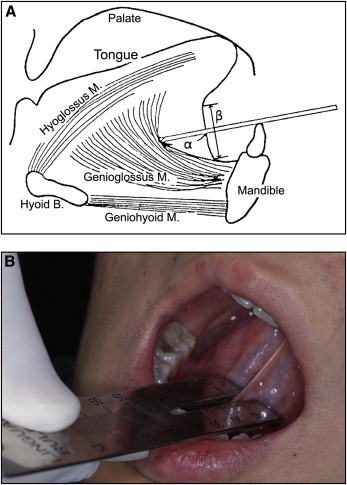
Ankyloglossia is a developmental anomaly of the tongue characterized by a short vertical lingual frenulum length ( Fig 1 , A ), which may result in a varying degree of decreased tongue tip mobility. The clinical consequences of ankyloglossia include infant breastfeeding difficulties, speech disorders, various mechanical and social issues related to the inability of the tongue movement, and orthodontic anomalies. Sometimes low tongue posture may cause a forward and downward pressure to the mandible with different consequences on face development.
Several clinical reports suggested that ankyloglossia may produce anterior open bite and mandibular protrusion malocclusions because of tongue posture. However, current literature regarding the lingual frenulum and tongue posture is scarce and has generally focused on the influence of the lingual frenulum in relation to dentoalveolar anomalies. The relationship between the lingual frenulum and craniofacial morphology has not been investigated. The purpose of this study was to determine if there is a relationship between the median lingual frenulum length and the craniofacial morphology. We hypothesize that the skeletal Class III malocclusion is related to the median lingual frenulum length and restricted mouth opening.
Material and methods
Patient sample
The sample was collected from the patients who were enrolled for orthodontic treatment at the Department of Orthodontics, Gangneung-Wonju National University Dental Hospital, Gangneung, South Korea. The selection criteria were as follows: no history of (1) previous lingual frenectomy, (2) previous orthodontic treatment, (3) previous orthognathic surgery, or (4) disorders of the temporomandibular joint and jaw-muscle. Based on the ANB angle, patients were classified as skeletal Class I (0° < ANB < 4°), skeletal Class II (ANB angle > 4°), and skeletal Class III (ANB angle < 0°) groups and each group has 50 patients. The distributions of age and ANB angle in different groups for all subjects are shown in Table I .
| Groups | Gender | n | Age (years) | ANB angle (degree) | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Class I | Male | 22 | 25.7 | 5.7 | 2.3 | 1.1 |
| Female | 28 | 23.3 | 5.5 | 2.2 | 1.1 | |
| Total | 50 | 24.4 | 5.7 | 2.2 | 1.1 | |
| Class II | Male | 21 | 25.1 | 6.5 | 5.1 | 1.3 |
| Female | 29 | 23.9 | 7.9 | 6.2 | 1.6 | |
| Total | 50 | 24.4 | 7.3 | 6.0 | 1.5 | |
| Class III | Male | 28 | 25.0 | 5.1 | -2.4 | 2.8 |
| Female | 22 | 27.1 | 8.9 | -1.9 | 2.0 | |
| Total | 50 | 25.9 | 7.0 | -2.2 | 2.4 | |
Length of the median lingual frenulum
The measurements of the lingual frenulum were made by measuring the median lingual frenulum length using a lingual frenulum ruler (Dong-A Pharmaceutical Co., Ltd., Seoul, Korea) according to the procedures proposed by Lee et al ( Fig 1 ). The patient was instructed to put the tip of his or her tongue on the incisive papilla, and open the mouth to the maximum gap. The median lingual frenulum length was measured as the isthmus of the ruler was fully inserted and the other side of the ruler was touched on the lower anterior teeth ( Fig 1 ). This measurement represented the maximum lingual frenulum length in the middle of the tongue-tie. To reduce the measurement error by hand pressure to the lingual frenulum, the length was recorded as the ruler was touched on the soft tissue as lightly as possible; the average value of triplicate measurements was also recorded.
Maximum mouth opening reduction
The amount of maximum mouth opening reduction was measured by using a digital caliper (Digimatic, Mitutoyo, Tokyo, Japan) with a resolution of 0.01 mm, a nominal capacity of 150 mm, as previously described by Marchesan. First, the patient was requested to open his or her mouth as widely as possible and the caliper was positioned so that its extremities were in contact with the incisal margins of the maxillary central incisor and the mandibular homolateral central incisor. The patient was then requested to put the tip of his or her tongue on the incisive papilla maintaining it on that point and to open the mouth again to the maximum gap. The support points for the digital caliper were the same. The reduced amount of maximum mouth opening was then calculated by the difference of the 2 measurements.
Cephalometric analysis
The lateral cephalograms were taken in habitual occlusion with the CX-90SP (Asahi Roentgen Ind. Co., Ltd., Japan) by using a standardized technique and fixed anode–midsagittal plane distance. No correction was made for the constant linear enlargement of 10%. The lateral cephalograms of each subject were traced on acetate paper by 1 examiner (S.J.J.) in order to minimize interexaminer error. Computer-assisted cephalometric analysis was carried out by means of a Numonics digitizer (Quick Ceph Systems, San Diego, Calif) and of Quick Ceph Image Pro software, version 4.4 (Quick Ceph Systems, San Diego, Calif). Table II shows the angular and linear measurements used in this study.
| Variables |
|---|
| Sagittal measurements |
| SNA angle (°) |
| SNB angle (°) |
| ANB angle (°) |
| Wits appraisal (mm) |
| Maxillary length (Co-A) (mm) |
| Mandibular length (Co-Pog) (mm) |
| Mandibular body length (Go-Me) (mm) |
| Point A to nasion perpendicular to FH plane (A-N perp) (mm) |
| Pogonion to nasion perpendicular to FH plane (Pog-N perp) (mm) |
| APDI |
| Vertical measurements |
| Mandibular plane angle (FH/MP) (°) |
| Occlusal plane angle (SN/OcclPl) (°) |
| Palatal plane angle (FH/PP) (°) |
| Gonial angle (Ar-Go-Me) (°) |
| Posterior facial height (S-Go) (mm) |
| Anterior facial height (N-Me) (mm) |
| Facial height ratio (S-Go/N-Me) |
| ODI |
| Dental measurements |
| Upper incisor inclination (U1/FH) (°) |
| Lower incisor inclination (IMPA) (°) |
| Edge of lower incisor to NB line distance (L1-NB) (mm) |
| Interincisal angle (°) |
Method errors
The reliability of the measurements of the lingual frenulum was determined on 20 randomly selected adults not included in this study. These adults were examined at intervals of 14 days, by using the same method as in the present investigation. Testing for the method error of all measurements was done with Dahlberg’s formula (method error = √∑d2/2n
∑ d 2 / 2 n
where d is the difference between 2 measurements of a pair, and n is the number of subjects). The method error of the measurements of the median lingual frenulum length and maximum mouth opening reduction was found to be 0.57 mm and 1.66 mm, respectively.
The reliability of the cephalometric measurements was assessed by the same examiner duplicating tracings on 20 randomly chosen cephalograms at intervals of 14 days. The method errors calculated with Dahlberg’s formula ranged from 0.17 to 0.94 mm for linear measurements and from 0.53° to 1.27° for the angular measurements.
Statistical analysis
The statistical analyses were carried out with the statistical software (SPSS for Windows, version 14.0, SPSS Inc, Chicago, Ill). The gender differences in each of 3 skeletal groups were tested by using the independent samples t test. The median lingual frenulum length and maximum mouth opening reduction of skeletal Class I, II, and III were compared through analysis of variance (ANOVA) and Scheffe test. Pearson correlation analysis was used to detect any relationship among the median lingual frenulum length, maximum mouth opening reduction, and cephalometric variables.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


